You might also like
- Neuropathic Pain Guidance April 2023 v1.2Document6 pagesNeuropathic Pain Guidance April 2023 v1.2Germán Bernate ObandoNo ratings yet
- Neuropathic Pain TreatmentDocument8 pagesNeuropathic Pain TreatmentIrimes MariaNo ratings yet
- Managing Patients With Chronic AnginaDocument10 pagesManaging Patients With Chronic Anginacindyfuller68No ratings yet
- Diabetic Peripheral Neuropathy Enhanced Primary Care Pathway FINAL Feb 7 2018 For PostingDocument4 pagesDiabetic Peripheral Neuropathy Enhanced Primary Care Pathway FINAL Feb 7 2018 For PostingNurul FajriNo ratings yet
- Neurontin (Gabapentin)Document1 pageNeurontin (Gabapentin)E100% (3)
- Ketorolac drug studyDocument2 pagesKetorolac drug studyJacqueline LimNo ratings yet
- Drug TylenolDocument1 pageDrug TylenolSrkocherNo ratings yet
- HeadacheDocument16 pagesHeadacheBagoes Ario BimoNo ratings yet
- NeurontinDocument1 pageNeurontinAdrianne BazoNo ratings yet
- Temazepam (Restoril)Document1 pageTemazepam (Restoril)Adrianne BazoNo ratings yet
- Temazepam (Restoril)Document1 pageTemazepam (Restoril)Adrianne BazoNo ratings yet
- Psychiatric Informed Consent - Augmented PsychotherapyDocument6 pagesPsychiatric Informed Consent - Augmented PsychotherapyNicolas Berasain OcaresNo ratings yet
- Migraine FlowchartDocument2 pagesMigraine FlowchartKemunto OnchwariNo ratings yet
- TylenolDocument1 pageTylenolCassieNo ratings yet
- Drug Study For AMCDocument3 pagesDrug Study For AMCTrixia RiveraNo ratings yet
- NURS 1566 Clinical Form 3: Clinical Medications WorksheetsDocument1 pageNURS 1566 Clinical Form 3: Clinical Medications WorksheetsCassieNo ratings yet
- Epilepsy Questions 2021Document5 pagesEpilepsy Questions 2021z_sadiqNo ratings yet
- NURS 5 Clinical Medications WorksheetsDocument1 pageNURS 5 Clinical Medications WorksheetsMichael KuzbytNo ratings yet
- NHS Pain Management Guide to AmitriptylineDocument8 pagesNHS Pain Management Guide to AmitriptylineteddypolNo ratings yet
- Drug Analysis AdultDocument4 pagesDrug Analysis AdultXian AlbsNo ratings yet
- 1 Neuropathic Pain AlgorithmDocument2 pages1 Neuropathic Pain AlgorithmRazmin SicatNo ratings yet
- Alprazolam (Systemic)Document14 pagesAlprazolam (Systemic)RIRINo ratings yet
- AcetaminophenDocument1 pageAcetaminophenKatie McPeek100% (1)
- What GPs Need To Know About KetamineDocument4 pagesWhat GPs Need To Know About KetamineAdiAri RosiuNo ratings yet
- DiarryDocument10 pagesDiarryVan Ryan CondenoNo ratings yet
- Hesi NR292 ESE Study GuideDocument16 pagesHesi NR292 ESE Study Guidenaijababy89100% (12)
- Ketamine Infusion For CRPS or Opioid Weaning GuidelineDocument14 pagesKetamine Infusion For CRPS or Opioid Weaning GuidelineAlia SandoQaNo ratings yet
- Efns Guideline On The Treatment of Tension-Type Headache - Report of An Efns Task ForceDocument33 pagesEfns Guideline On The Treatment of Tension-Type Headache - Report of An Efns Task ForcecindyNo ratings yet
- PrazosinDocument1 pagePrazosinKatie McPeek0% (1)
- EVALUATION AND PROPHYLAXIS OF MIGRAINEDocument53 pagesEVALUATION AND PROPHYLAXIS OF MIGRAINEnesya_fanniaNo ratings yet
- Treating Diabetic Neuropathic Pain: Am Fam Physician. 2010 82 (2) :151-158. Katie Marchington PGY-2Document22 pagesTreating Diabetic Neuropathic Pain: Am Fam Physician. 2010 82 (2) :151-158. Katie Marchington PGY-2gjgibson2784No ratings yet
- Pudendal Nerve BlockDocument3 pagesPudendal Nerve BlockLauraNo ratings yet
- 19.07.12 - SENT - PA - CP.PMN.33 Pregabalin (Lyrica)Document9 pages19.07.12 - SENT - PA - CP.PMN.33 Pregabalin (Lyrica)ThiruNo ratings yet
- ZofranDocument1 pageZofranKatie McPeek0% (1)
- Pregabalin Leaflet 2022Document4 pagesPregabalin Leaflet 2022hautpflege.con.tatyNo ratings yet
- Drug Card AcetaminophenDocument1 pageDrug Card AcetaminophenAdrianne Bazo100% (3)
- Toradol KetorolacDocument2 pagesToradol KetorolacE100% (4)
- Protocol-010Document12 pagesProtocol-010hatem newishyNo ratings yet
- Drug AtivanDocument1 pageDrug AtivanSrkocherNo ratings yet
- Prozac (Fluoxetine) 40mgDocument1 pageProzac (Fluoxetine) 40mgENo ratings yet
- Practical Insulin: A Handbook for Prescribing ProvidersFrom EverandPractical Insulin: A Handbook for Prescribing ProvidersRating: 5 out of 5 stars5/5 (2)
- Psychiatry Practice Boosters, Second Edition: Insights from research to enhance your clinical workFrom EverandPsychiatry Practice Boosters, Second Edition: Insights from research to enhance your clinical workNo ratings yet
- Occipital Neuralgia: A Beginner's Guide and Overview to Managing the Condition Through Diet, with Sample Curated RecipesFrom EverandOccipital Neuralgia: A Beginner's Guide and Overview to Managing the Condition Through Diet, with Sample Curated RecipesNo ratings yet
- Trigeminal Neuralgia: A Beginner's 3-Step Quick Start Guide to Managing TB Through Diet, With Sample RecipesFrom EverandTrigeminal Neuralgia: A Beginner's 3-Step Quick Start Guide to Managing TB Through Diet, With Sample RecipesNo ratings yet
- Psychiatry Practice Boosters 2016: Insights from research to enhance your clinical workFrom EverandPsychiatry Practice Boosters 2016: Insights from research to enhance your clinical workNo ratings yet
- Arthritis: Medical, Alternative, and Complementary Treatments: The most important information you need to improve your healthFrom EverandArthritis: Medical, Alternative, and Complementary Treatments: The most important information you need to improve your healthNo ratings yet
- Keto Migraine: A Beginner's Quick Start Guide for Women on Managing Migraines Through the Ketogenic Diet, With Sample Curated RecipesFrom EverandKeto Migraine: A Beginner's Quick Start Guide for Women on Managing Migraines Through the Ketogenic Diet, With Sample Curated RecipesNo ratings yet
- Migraines and Epilepsy: How to Find Relief, Live Well, and Protect Your BrainFrom EverandMigraines and Epilepsy: How to Find Relief, Live Well, and Protect Your BrainNo ratings yet
- Postherpetic Neuralgia: A Beginner's Quick Start Guide to Managing Shingles Through Diet, With Sample Curated RecipesFrom EverandPostherpetic Neuralgia: A Beginner's Quick Start Guide to Managing Shingles Through Diet, With Sample Curated RecipesNo ratings yet
- Adrenal Fatigue: Adrenal Reset Diet: Understand The Symptoms And Beat Adrenal Fatigue Syndrome Forever. Lose Weight,Reduce Both Stress And Anxiety To Boost Vitality, Health And Energy LevelsFrom EverandAdrenal Fatigue: Adrenal Reset Diet: Understand The Symptoms And Beat Adrenal Fatigue Syndrome Forever. Lose Weight,Reduce Both Stress And Anxiety To Boost Vitality, Health And Energy LevelsRating: 1 out of 5 stars1/5 (1)
- Step 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionFrom EverandStep 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionNo ratings yet
- Your Best Brain: Discover the Secrets to Biohacking Maximum Mental PerformanceFrom EverandYour Best Brain: Discover the Secrets to Biohacking Maximum Mental PerformanceNo ratings yet
- Vagus Nerve Diet: A Beginner's 3-Week Step-by-Step Guide to Managing Anxiety, Inflammation, and Depression Through Diet, With Sample Recipes and a Meal PlanFrom EverandVagus Nerve Diet: A Beginner's 3-Week Step-by-Step Guide to Managing Anxiety, Inflammation, and Depression Through Diet, With Sample Recipes and a Meal PlanNo ratings yet
- Diabetes: Glucose Monitoring and Insulin Treatment: The most important information you need to improve your healthFrom EverandDiabetes: Glucose Monitoring and Insulin Treatment: The most important information you need to improve your healthNo ratings yet
- RMO Skills ListDocument2 pagesRMO Skills ListHenrypat Uche OgbuduNo ratings yet
- 2013AminoglycosideDosingGuide PDFDocument2 pages2013AminoglycosideDosingGuide PDFFelipe SotoNo ratings yet
- Statemenu Purpose PDFDocument2 pagesStatemenu Purpose PDFHenrypat Uche OgbuduNo ratings yet
- Synonyms For Words Commonly UsedDocument5 pagesSynonyms For Words Commonly UsedEricDenby100% (19)
- FormDocument7 pagesFormHenrypat Uche OgbuduNo ratings yet
- PLAB Topics To Be CoveredDocument8 pagesPLAB Topics To Be CoveredHenrypat Uche OgbuduNo ratings yet
- What To Do After PlabDocument2 pagesWhat To Do After PlabnaeamzNo ratings yet
- RMO Skills ListDocument1 pageRMO Skills ListHenrypat Uche OgbuduNo ratings yet
- Requirements VisaDocument2 pagesRequirements VisaHenrypat Uche OgbuduNo ratings yet
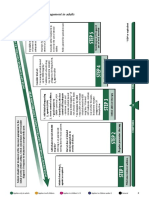
- Summary of Stepwise Management in AdultsDocument3 pagesSummary of Stepwise Management in AdultsHenrypat Uche OgbuduNo ratings yet
- Introducing Dung Beetles to PasturesDocument3 pagesIntroducing Dung Beetles to PasturesdarylNo ratings yet
- Statement U PurposeDocument2 pagesStatement U PurposeHenrypat Uche Ogbudu100% (1)
- Psychiatry Imp Topics & NotesDocument4 pagesPsychiatry Imp Topics & NotesHenrypat Uche OgbuduNo ratings yet
- INTERNAL MEDICINE Imp Topics PDFDocument6 pagesINTERNAL MEDICINE Imp Topics PDFHenrypat Uche OgbuduNo ratings yet
- AndreDocument8 pagesAndreHenrypat Uche OgbuduNo ratings yet
- GMC Specimen Questions For PLABDocument8 pagesGMC Specimen Questions For PLABHenrypat Uche OgbuduNo ratings yet
- PLAB Obs Gyne MCQsDocument33 pagesPLAB Obs Gyne MCQsHenrypat Uche Ogbudu100% (3)
- July 2004 Sbas Plab Emqs SbaDocument12 pagesJuly 2004 Sbas Plab Emqs SbaDrZahir UmarNo ratings yet
- Abia State UniversityDocument1 pageAbia State UniversityHenrypat Uche OgbuduNo ratings yet
- AbstractDocument1 pageAbstractHenrypat Uche OgbuduNo ratings yet
- Application Letter - ST NicholasDocument1 pageApplication Letter - ST NicholasHenrypat Uche OgbuduNo ratings yet
- Last TypedDocument2 pagesLast TypedHenrypat Uche OgbuduNo ratings yet
- Professional TrainingDocument1 pageProfessional TrainingHenrypat Uche OgbuduNo ratings yet
- PC Keyboard Shortcuts PDFDocument1 pagePC Keyboard Shortcuts PDFSelvaraj VillyNo ratings yet
- Print TotalDocument1 pagePrint TotalHenrypat Uche OgbuduNo ratings yet
- Scope of HRM: 1. The Labour or Personnel AspectDocument4 pagesScope of HRM: 1. The Labour or Personnel AspectHenrypat Uche OgbuduNo ratings yet
- International Financial Questionnaire (IFQ) FormDocument4 pagesInternational Financial Questionnaire (IFQ) FormHenrypat Uche Ogbudu100% (1)
- Professional TrainingDocument1 pageProfessional TrainingHenrypat Uche OgbuduNo ratings yet
- NDDC Foreign Scholarship ProgramDocument2 pagesNDDC Foreign Scholarship ProgramHenrypat Uche Ogbudu100% (1)