You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- VocabMagik - Fall in Love With Vocabulary!Document106 pagesVocabMagik - Fall in Love With Vocabulary!VocabMagiikNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Absolute Hospital Medicine ReviewDocument213 pagesAbsolute Hospital Medicine ReviewLuis Daniel Bernal Conde83% (6)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Company ProfileDocument11 pagesCompany Profilejen100% (3)
- Cholelithiasis Case StudyDocument13 pagesCholelithiasis Case StudyJoshua PayawalNo ratings yet
- Planning and Designing An Isolation Facility in Hospitals Need of The Hour PDFDocument9 pagesPlanning and Designing An Isolation Facility in Hospitals Need of The Hour PDFdzakyzahidNo ratings yet
- Mae Geraldine Valeza Samar, BSN, RN: Career ObjectiveDocument4 pagesMae Geraldine Valeza Samar, BSN, RN: Career ObjectiveJackie Lou DimatulacNo ratings yet
- Vivapore FlyerDocument1 pageVivapore FlyerDesak PramestiNo ratings yet
- Vivamel FlyerDocument1 pageVivamel FlyerDesak PramestiNo ratings yet
- Postoperative Peritoneal Adhesions in Adults and Their Prevention - UpToDateDocument17 pagesPostoperative Peritoneal Adhesions in Adults and Their Prevention - UpToDateDesak PramestiNo ratings yet
- Overview of Management of Mechanical Small Bowel Obstruction in Adults - UpToDateDocument19 pagesOverview of Management of Mechanical Small Bowel Obstruction in Adults - UpToDateDesak PramestiNo ratings yet
- 1 s2.0 S0022346812003818 MainDocument2 pages1 s2.0 S0022346812003818 MainDesak PramestiNo ratings yet
- bcr2831 PDFDocument9 pagesbcr2831 PDFDesak PramestiNo ratings yet
- Initial Evaluation and Management of Abdominal Stab Wounds in Adults - UpToDateDocument19 pagesInitial Evaluation and Management of Abdominal Stab Wounds in Adults - UpToDateDesak PramestiNo ratings yet
- Cole GuidelineDocument14 pagesCole GuidelinePratita Jati PermatasariNo ratings yet
- Daftar Acara Trigonum Xli (Trawas 24-27 Nop 2016)Document2 pagesDaftar Acara Trigonum Xli (Trawas 24-27 Nop 2016)Desak PramestiNo ratings yet
- Bang BangDocument4 pagesBang BangDesak PramestiNo ratings yet
- Accepted Manuscript: 10.1016/j.cjtee.2015.12.015Document8 pagesAccepted Manuscript: 10.1016/j.cjtee.2015.12.015Desak PramestiNo ratings yet
- Upj Ped DidacticDocument24 pagesUpj Ped DidacticDesak PramestiNo ratings yet
- Man On Wire ChordsDocument3 pagesMan On Wire ChordsDesak PramestiNo ratings yet
- Eem Education Session3Document21 pagesEem Education Session3Gama AntaresNo ratings yet
- Germany RconomyDocument11 pagesGermany RconomyDesak PramestiNo ratings yet
- Route MapDocument1 pageRoute MapTerence LeungNo ratings yet
- NEL230402R04 Lewinski RWDocument5 pagesNEL230402R04 Lewinski RWDesak PramestiNo ratings yet
- Garry Billy PDEDocument1 pageGarry Billy PDEDesak PramestiNo ratings yet
- Full Guidelines ManuscriptDocument44 pagesFull Guidelines ManuscriptDesak PramestiNo ratings yet
- Chapter 1Document4 pagesChapter 1Desak PramestiNo ratings yet
- HSP 5Document8 pagesHSP 5Desak PramestiNo ratings yet
- Estrogen Receptor, Progesterone Receptor, and HER-2/neu Protein in Breast Cancers From Pregnant PatientsDocument8 pagesEstrogen Receptor, Progesterone Receptor, and HER-2/neu Protein in Breast Cancers From Pregnant PatientsDesak PramestiNo ratings yet
- Annotated BibDocument4 pagesAnnotated BibAmelia ArnisNo ratings yet
- Algorithm 1. Use of PE Criteria Based On Patient Location at Time of EventDocument5 pagesAlgorithm 1. Use of PE Criteria Based On Patient Location at Time of EventKatherynSotoNo ratings yet
- Philippines Health System ReviewDocument166 pagesPhilippines Health System ReviewAgripino Agulo JrNo ratings yet
- Children's Services Job DescriptionDocument11 pagesChildren's Services Job DescriptionMuhammad Dian Luthfy LubisNo ratings yet
- Leg Med SummerDocument69 pagesLeg Med SummerMichael Angelo MemoracionNo ratings yet
- Notification PDFDocument3 pagesNotification PDFAnonymous BDrXXkNo ratings yet
- Patient Pictogram RubricDocument3 pagesPatient Pictogram Rubricapi-320828853No ratings yet
- Agusan Del Norte Provincial Hospital: Memorandum No. 224Document2 pagesAgusan Del Norte Provincial Hospital: Memorandum No. 224Pia Mae BuayaNo ratings yet
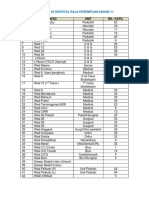
- Senarai Wad Dan KlinikDocument2 pagesSenarai Wad Dan Klinikfarhyn1991No ratings yet
- Davina Saltos ResumeDocument1 pageDavina Saltos ResumeDavina SaltosNo ratings yet
- Diana Rose Verzosa Paunan: #20 N. Ramirez St. Barangay Don Manuel Quezon City PhilippinesDocument3 pagesDiana Rose Verzosa Paunan: #20 N. Ramirez St. Barangay Don Manuel Quezon City PhilippinesGloria Verzosa Paunan100% (1)
- Nurs 406 e FolioDocument4 pagesNurs 406 e Folioapi-273787321No ratings yet
- Coffee Table Book - Naya RaipurDocument19 pagesCoffee Table Book - Naya RaipurAmitomSudarshanNo ratings yet
- Arianne C. DizonDocument3 pagesArianne C. DizonAira DizonNo ratings yet
- Memorial For AppellantDocument17 pagesMemorial For AppellantKandlagunta Gayathri PraharshithaNo ratings yet
- Benefit Guide AllianzDocument50 pagesBenefit Guide AllianzAbstractSoftNo ratings yet
- Chest Drains Al-WPS OfficeDocument16 pagesChest Drains Al-WPS OfficeisnainiviaNo ratings yet
- Cisto PilonidalDocument4 pagesCisto PilonidalGuilherme Diogo GesualdoNo ratings yet
- B Bartholins Abscess - Word CatheterDocument2 pagesB Bartholins Abscess - Word CatheterMuhammadUsriYusranNo ratings yet
- Tugas Bahasa Inggris 2 Per 1Document4 pagesTugas Bahasa Inggris 2 Per 1Rori RevizaNo ratings yet
- NOVADAQ Corporate Presentation May 2015 - 0Document27 pagesNOVADAQ Corporate Presentation May 2015 - 0medtechyNo ratings yet
- Vulnerable Population PaperDocument7 pagesVulnerable Population Paperapi-253602771No ratings yet
- McKenzie Aasfe 1st Place Division2Document23 pagesMcKenzie Aasfe 1st Place Division2Margaret McKenzieNo ratings yet
- Agreement AmbulanceDocument3 pagesAgreement AmbulanceVIKAS PANERI100% (2)