You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Neonatal Air Leak Syndrome and The Role Of.3Document9 pagesNeonatal Air Leak Syndrome and The Role Of.3Claudia KosztelnikNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Mechanical Ventilation Guidelines SNSDocument8 pagesMechanical Ventilation Guidelines SNSClaudia KosztelnikNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Imaging Findings in Cardiac Tamponade With EmphasiDocument18 pagesImaging Findings in Cardiac Tamponade With EmphasiClaudia KosztelnikNo ratings yet
- Lung Ultrasound For Neonatal Cardio-Respiratory Conditions: Daniele de Luca (MD, PHD)Document52 pagesLung Ultrasound For Neonatal Cardio-Respiratory Conditions: Daniele de Luca (MD, PHD)Claudia Kosztelnik100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- 03 - Special Clinical SituationsDocument32 pages03 - Special Clinical SituationsClaudia KosztelnikNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- User Guide: IBM Micromedex® Neofax® and PediatricsDocument57 pagesUser Guide: IBM Micromedex® Neofax® and PediatricsClaudia KosztelnikNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 406ronmfrt0n7269301 PDFDocument5 pages406ronmfrt0n7269301 PDFClaudia KosztelnikNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- High DoseDocument6 pagesHigh DoseClaudia KosztelnikNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- LAPTARE Copii Cu Patologie...Document8 pagesLAPTARE Copii Cu Patologie...Claudia KosztelnikNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Evolution of NeonatologyDocument17 pagesEvolution of NeonatologyClaudia KosztelnikNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
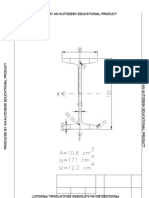
- Produced by An Autodesk Educational ProductDocument1 pageProduced by An Autodesk Educational ProductClaudia KosztelnikNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Assessment Nursing Diagnosis Scientific Explanation Goal of Care Intervention Rationale EvaluationDocument4 pagesAssessment Nursing Diagnosis Scientific Explanation Goal of Care Intervention Rationale EvaluationHowel CristobalNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Topic 9 Cardiovascular SystemDocument36 pagesTopic 9 Cardiovascular SystemAlejandra CastilloNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Basics of EKG Interpretation: Michael Rochon-Duck July 6, 2015 Slideset Adapted From: Jennifer Ballard-Hernandez, DNPDocument127 pagesBasics of EKG Interpretation: Michael Rochon-Duck July 6, 2015 Slideset Adapted From: Jennifer Ballard-Hernandez, DNPYS NateNo ratings yet
- Critical Care NursingDocument17 pagesCritical Care Nursingsanish4u100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Focused Ultrasonography For Septic Shock ResuscitationDocument7 pagesFocused Ultrasonography For Septic Shock ResuscitationntnquynhproNo ratings yet
- CC-Chronic Venous Insufficiency ArticleDocument24 pagesCC-Chronic Venous Insufficiency ArticleGutierrez MarinellNo ratings yet
- Rotational Atherectomy - WikidocDocument2 pagesRotational Atherectomy - WikidocnarasaiyanhariharanNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Chapter 10 - Web Quiz 1Document4 pagesChapter 10 - Web Quiz 1Nicky PhakathiNo ratings yet
- Ecg Heart Sounds Laboratory HandoutDocument7 pagesEcg Heart Sounds Laboratory HandoutShashank SahuNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Nursing Care Plan For Coronary Artery DiseaseDocument3 pagesNursing Care Plan For Coronary Artery DiseaseLorraineAnneSantiagoCandelario91% (22)
- Case Presentation-Neonatal SepsisDocument22 pagesCase Presentation-Neonatal SepsisDianne Dawn0% (1)
- Session #33 SAS - AnaPhy (Lab)Document5 pagesSession #33 SAS - AnaPhy (Lab)G INo ratings yet
- Chapter8-Transport in HumansDocument15 pagesChapter8-Transport in HumansミーチェルNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- IJARDoppler Ultrasonography AbdominalvesselsDocument6 pagesIJARDoppler Ultrasonography AbdominalvesselsDr.Lázár AttilaNo ratings yet
- DLL March 26 - Ailments of The Respiratory and Circulatroy SystemDocument4 pagesDLL March 26 - Ailments of The Respiratory and Circulatroy Systemirah jane valentinoNo ratings yet
- ECG ProjectDocument58 pagesECG Projectد. سعد قاسم الاجهزة الطبيةNo ratings yet
- Training Manual For Medical RepresentativesDocument74 pagesTraining Manual For Medical RepresentativesAman Ghayas50% (4)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Care of Patient With TPM Slide PresentationDocument16 pagesCare of Patient With TPM Slide PresentationirzehronNo ratings yet
- Discovery of The Blood CirculationDocument17 pagesDiscovery of The Blood CirculationSaim BaigNo ratings yet
- The Coronary CirculationDocument12 pagesThe Coronary CirculationJulia PutnikNo ratings yet
- Fellowship in Clinical CardiologyDocument6 pagesFellowship in Clinical CardiologysulatnazeemNo ratings yet
- Task 2: Physiological Exercise and Physical Activity: To Transport Nutrients, Gases and Waste Products Around The BodyDocument2 pagesTask 2: Physiological Exercise and Physical Activity: To Transport Nutrients, Gases and Waste Products Around The Bodyjohn paul PatronNo ratings yet
- The Dog Encyclopedia (VetBooks - Ir)Document362 pagesThe Dog Encyclopedia (VetBooks - Ir)miki122295% (22)
- Quiz - CardiovascularDocument4 pagesQuiz - CardiovascularRebekah HNo ratings yet
- Circulatory System FKM'12Document55 pagesCirculatory System FKM'12muhammadsudrajadNo ratings yet
- Diagnostic Pacing Maneuvers For Supraventricular Tachycardia - Part 2Document13 pagesDiagnostic Pacing Maneuvers For Supraventricular Tachycardia - Part 2aafagihNo ratings yet
- CardioDocument507 pagesCardioSdoc0% (1)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 7040 GCE O Biology MSC 20080807Document30 pages7040 GCE O Biology MSC 20080807Mehjabeen HossainNo ratings yet
- Ecg - AclsDocument338 pagesEcg - AclsPete Cobra CobraitiNo ratings yet
- Syllabus: Cambridge O Level Biology 5090Document46 pagesSyllabus: Cambridge O Level Biology 5090Sayma AkterNo ratings yet