You might also like
- Condiloma AkuminataDocument3 pagesCondiloma AkuminataAlmas PrawotoNo ratings yet
- Cutaneous Changes in Venous and Lymphatic InsufficiencyDocument4 pagesCutaneous Changes in Venous and Lymphatic InsufficiencyAlmas PrawotoNo ratings yet
- Condiloma AkuminataDocument3 pagesCondiloma AkuminataAlmas PrawotoNo ratings yet
- Why Is Long-Term Therapy Required To Cure Tuberculosis?: Research in TranslationDocument8 pagesWhy Is Long-Term Therapy Required To Cure Tuberculosis?: Research in TranslationMonica Herdiati Rukmana NaibahoNo ratings yet
- Perioperative Planning & Pain ManagementDocument18 pagesPerioperative Planning & Pain ManagementAlmas PrawotoNo ratings yet
- Journal Reading IKK ANHDocument15 pagesJournal Reading IKK ANHAlmas PrawotoNo ratings yet
- Identifying Risk For Diabetes in Adolescence (Irda) : A Pilot Study in General PracticeDocument12 pagesIdentifying Risk For Diabetes in Adolescence (Irda) : A Pilot Study in General PracticeAlmas PrawotoNo ratings yet
- Hawaii Hotel NumberDocument1 pageHawaii Hotel NumberAlmas PrawotoNo ratings yet
- Diabetes in TeensDocument5 pagesDiabetes in TeensAlmas PrawotoNo ratings yet
- Bab 1Document2 pagesBab 1Almas PrawotoNo ratings yet
- Oxford Perioperative Pain Management 2013Document141 pagesOxford Perioperative Pain Management 2013Almas PrawotoNo ratings yet
- Hawaii Travel PlanDocument103 pagesHawaii Travel PlanAlmas PrawotoNo ratings yet
- Interpretasi RontgenDocument12 pagesInterpretasi RontgenAlmas PrawotoNo ratings yet
- Journal Ischemic StrokeDocument9 pagesJournal Ischemic StrokeAlmas PrawotoNo ratings yet
- Side Effects of NSAIDsDocument8 pagesSide Effects of NSAIDsAlmas PrawotoNo ratings yet
- Fracture ManagementDocument4 pagesFracture ManagementAlmas PrawotoNo ratings yet
- Hidronefrosis PDFDocument54 pagesHidronefrosis PDFAlmas PrawotoNo ratings yet
- Guideline PresbycusisDocument4 pagesGuideline PresbycusisAlmas PrawotoNo ratings yet
- Damage ControlDocument8 pagesDamage ControlAlmas PrawotoNo ratings yet
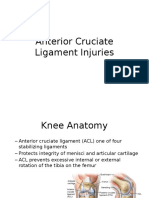
- Anterior Cruciate Ligament InjuriesDocument16 pagesAnterior Cruciate Ligament InjuriesAlmas PrawotoNo ratings yet
- Official Reprint From Uptodate ©2017 UptodateDocument9 pagesOfficial Reprint From Uptodate ©2017 UptodateAlmas Prawoto100% (1)
- OsteomyelitisDocument5 pagesOsteomyelitisAlmas PrawotoNo ratings yet
- Meniscus Injury: Almas PrawotoDocument9 pagesMeniscus Injury: Almas PrawotoAlmas PrawotoNo ratings yet
- Post TraumaDocument5 pagesPost TraumaAlmas PrawotoNo ratings yet
- Fracture ManagementDocument4 pagesFracture ManagementAlmas PrawotoNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- What Does A Piano Tuner Do When He Goes Deaf PDFDocument4 pagesWhat Does A Piano Tuner Do When He Goes Deaf PDFSpencer GrahamNo ratings yet
- Otitis MediaDocument11 pagesOtitis MediajessyNo ratings yet
- Otomycosis With Tympanic Membrane Perforation: A Review of The LiteratureDocument4 pagesOtomycosis With Tympanic Membrane Perforation: A Review of The Literaturekhusna wahyuniNo ratings yet
- Intraauricular AbscessDocument15 pagesIntraauricular AbscessromaNo ratings yet
- Music Therapy PsychiatryDocument59 pagesMusic Therapy PsychiatryAlberto ChicaybanNo ratings yet
- Foto Acoustic EmitionDocument83 pagesFoto Acoustic EmitionAlok kumarNo ratings yet
- Audiometric SymbolsDocument15 pagesAudiometric SymbolsNicolás Molina TapiaNo ratings yet
- Manual of Temporal Bone DissectionDocument82 pagesManual of Temporal Bone DissectionBungbu Tn100% (3)
- Form 2 Chapter 1Document6 pagesForm 2 Chapter 1naza977562% (13)
- filePV 27 05 377Document9 pagesfilePV 27 05 377pifmanNo ratings yet
- 13 Cognitive Biases and MusicDocument20 pages13 Cognitive Biases and MusicJacinta SmithNo ratings yet
- Mayo Clinic BPPVDocument4 pagesMayo Clinic BPPVCS NarayananNo ratings yet
- Health Science - Healthy EarsDocument11 pagesHealth Science - Healthy Earsapi-583392653No ratings yet
- OtosclerosisDocument46 pagesOtosclerosisMariana CabralNo ratings yet
- Assessment of HearingDocument30 pagesAssessment of HearingNitin SharmaNo ratings yet
- Understanding Eye Anatomy and Common Eye DisordersDocument174 pagesUnderstanding Eye Anatomy and Common Eye DisordersroseNo ratings yet
- S LUPESCU Timpanoplastia Under OverlayDocument109 pagesS LUPESCU Timpanoplastia Under OverlayEdy MorarNo ratings yet
- Adhi Wardana 405120042: Blok PenginderaanDocument51 pagesAdhi Wardana 405120042: Blok PenginderaanErwin DiprajaNo ratings yet
- AP Psychology Review in 40 CharactersDocument83 pagesAP Psychology Review in 40 CharactersKitty chenNo ratings yet
- Earmolds ManualDocument97 pagesEarmolds ManualdawksNo ratings yet
- Management of Vertigo - DR - Attiya Rahma SpsDocument59 pagesManagement of Vertigo - DR - Attiya Rahma SpsHenni Pus Vera100% (1)
- The Basic Theory of Mind and MatterDocument24 pagesThe Basic Theory of Mind and MatterJhayar BernNo ratings yet
- 2019 International Symposium on Pediatric Audiology ScheduleDocument3 pages2019 International Symposium on Pediatric Audiology ScheduleEulalia JuanNo ratings yet
- Vestibulo Cochlear AppDocument35 pagesVestibulo Cochlear AppApi Rosela AlfiNo ratings yet
- Assessment of The Ears Rev 4-2013Document8 pagesAssessment of The Ears Rev 4-2013alphabennydelta4468No ratings yet
- Tinnitus Today September 2001 Vol 26, No 3Document27 pagesTinnitus Today September 2001 Vol 26, No 3American Tinnitus AssociationNo ratings yet
- CH 4 Notes Sensation and PerceptionDocument99 pagesCH 4 Notes Sensation and Perceptionapi-261300427No ratings yet
- Asymmetrical Hearing Loss: Jessica PrasadDocument6 pagesAsymmetrical Hearing Loss: Jessica PrasadSujaya ChattopadhyayNo ratings yet
- Hennebert's SignDocument3 pagesHennebert's SignatmhyaNo ratings yet
- Ayurvedic Approach to Vertigo, Hearing Loss and TinnitusDocument5 pagesAyurvedic Approach to Vertigo, Hearing Loss and TinnitusAmmiraju Gorti ChoudharyNo ratings yet