You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Atcmorse PDFDocument50 pagesAtcmorse PDFdivyansh bansalNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elements of HardscapingDocument57 pagesElements of HardscapingNathar ShaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Specifications: Louie Jean Mabanag Ar - 3BDocument8 pagesSpecifications: Louie Jean Mabanag Ar - 3BLouie Jean100% (1)
- Risk Assesment FOR PIPING WORKDocument1 pageRisk Assesment FOR PIPING WORKsunil100% (2)
- Booster Mock Test For NEETDocument15 pagesBooster Mock Test For NEETDrNo ratings yet
- Bright Ideas 2 Unit 1 Test-Fusionado-Páginas-1-33Document33 pagesBright Ideas 2 Unit 1 Test-Fusionado-Páginas-1-33Eleonora Graziano100% (1)
- BFD-180-570 DN65 GBDocument25 pagesBFD-180-570 DN65 GBalexander100% (3)
- GuidelineShock PDFDocument9 pagesGuidelineShock PDFValentina Lakhsmi PrabandariNo ratings yet
- Shock: A Review of Pathophysiology and Management. Part II: L. I. G. WorthleyDocument19 pagesShock: A Review of Pathophysiology and Management. Part II: L. I. G. Worthleynutnut_chanNo ratings yet
- GuidelineShock PDFDocument9 pagesGuidelineShock PDFValentina Lakhsmi PrabandariNo ratings yet
- Thinking Out LoudDocument1 pageThinking Out LoudGabrielaGeorgianaNo ratings yet
- Resusitasi Cairan PD Syok HipovolemikDocument4 pagesResusitasi Cairan PD Syok HipovolemikValentina Lakhsmi PrabandariNo ratings yet
- Syndrome Cleft Lip and PalateDocument8 pagesSyndrome Cleft Lip and PalateValentina Lakhsmi PrabandariNo ratings yet
- Revascularization On Cardiogenic ShockDocument3 pagesRevascularization On Cardiogenic ShockValentina Lakhsmi PrabandariNo ratings yet
- Trauma AbdominalDocument12 pagesTrauma AbdominalmelmeldidiNo ratings yet
- 2012-01-25 Cupping Brochure 2Document2 pages2012-01-25 Cupping Brochure 2Valentina Lakhsmi PrabandariNo ratings yet
- Syndrome Cleft Lip and PalateDocument8 pagesSyndrome Cleft Lip and PalateValentina Lakhsmi PrabandariNo ratings yet
- Guideline 9 2 3feb09 Shock TherapyDocument2 pagesGuideline 9 2 3feb09 Shock TherapyValentina Lakhsmi PrabandariNo ratings yet
- Safe and Gentle Ventilation For Little Patients Easy - Light - SmartDocument4 pagesSafe and Gentle Ventilation For Little Patients Easy - Light - SmartSteven BrownNo ratings yet
- Concrete Tunnel Design and Calculation Spreadsheet Based On AASHTO and ACIDocument3 pagesConcrete Tunnel Design and Calculation Spreadsheet Based On AASHTO and ACIFirat PulatNo ratings yet
- Sri Vidya College of Engineering & Technology Virudhunagar: Department: Semester: Vi SUBJECT CODE / Name: CE 6602Document34 pagesSri Vidya College of Engineering & Technology Virudhunagar: Department: Semester: Vi SUBJECT CODE / Name: CE 6602JEYA KUMARNo ratings yet
- Evolution of Indian TolucaDocument28 pagesEvolution of Indian TolucaAlberto Duran IniestraNo ratings yet
- Slides Arrays Two Dimensional ArraysDocument12 pagesSlides Arrays Two Dimensional ArraysPratham MishraNo ratings yet
- Assignment Oumh2103 English For Science Technical PurposesDocument12 pagesAssignment Oumh2103 English For Science Technical PurposesKhairul AnuarNo ratings yet
- 5980 10143 1 SM PDFDocument11 pages5980 10143 1 SM PDFfaustinaNo ratings yet
- Baccano! NDS 1931 The Grand Punk Railroad Secret EpisodeDocument38 pagesBaccano! NDS 1931 The Grand Punk Railroad Secret EpisodeAymen AlhajNo ratings yet
- Mat11 PDFDocument13 pagesMat11 PDFRaquel Martins E SilvaNo ratings yet
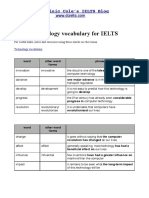
- Technology VocabularyDocument3 pagesTechnology VocabularyChixo GalaxyNo ratings yet
- MPL Construction PDFDocument40 pagesMPL Construction PDFSheraz QamerNo ratings yet
- PVC Duct DesignDocument10 pagesPVC Duct DesigncitramuaraNo ratings yet
- Coronary Stents: Current StatusDocument42 pagesCoronary Stents: Current StatusMANSI SALUNKENo ratings yet
- Covid 19Document1 pageCovid 19Sadiq NaseerNo ratings yet
- GIRBESDocument6 pagesGIRBESMiguel LópezNo ratings yet
- A Report On External Analysis of Construction in NepalDocument13 pagesA Report On External Analysis of Construction in Nepalsubash upretiNo ratings yet
- Review Questions UAPGADocument28 pagesReview Questions UAPGAkarenNo ratings yet
- AidsDocument22 pagesAidsVicky Singh100% (2)
- Synthesis of Sentences Is The Opposite ofDocument9 pagesSynthesis of Sentences Is The Opposite ofSpsc AspirantsNo ratings yet
- Cantece Copii in EnglezaDocument10 pagesCantece Copii in EnglezaGeorgi Neacşa100% (1)
- Feeg2003 L21Document9 pagesFeeg2003 L21jiales225No ratings yet
- ED1021 - I/O Expander With UART Interface & Analog Inputs: PreliminaryDocument9 pagesED1021 - I/O Expander With UART Interface & Analog Inputs: PreliminaryMilan NovakovićNo ratings yet