You might also like
- LSD OD 1975 - Klock - 3266 - 1Document13 pagesLSD OD 1975 - Klock - 3266 - 10j1u9nmkv534vw9vNo ratings yet
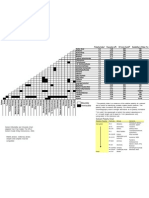
- Solvent Miscibility and Polarity ChartDocument1 pageSolvent Miscibility and Polarity Chartdiptafara100% (3)
- Coma, Hyperthermia and Bleeding Associated With Massive LSD OverdoseDocument6 pagesComa, Hyperthermia and Bleeding Associated With Massive LSD Overdose0j1u9nmkv534vw9vNo ratings yet
- King Scientific CatalogueDocument694 pagesKing Scientific Catalogue0j1u9nmkv534vw9v100% (1)
- Pressure Conversion TableDocument1 pagePressure Conversion Table0j1u9nmkv534vw9vNo ratings yet
- Synthesis of Amides of Lysergic AcidDocument5 pagesSynthesis of Amides of Lysergic Acid0j1u9nmkv534vw9v100% (1)
- LSD and Its Lysergamide CousinsDocument8 pagesLSD and Its Lysergamide Cousins0j1u9nmkv534vw9vNo ratings yet
- The Characterization of 2 - (3-Methoxyphenyl) - 2 - (Ethylamino) Cyclohexanone (Methoxetamine)Document15 pagesThe Characterization of 2 - (3-Methoxyphenyl) - 2 - (Ethylamino) Cyclohexanone (Methoxetamine)0j1u9nmkv534vw9vNo ratings yet
- UK Government Drug Precursors Wallchart Update February 2012Document2 pagesUK Government Drug Precursors Wallchart Update February 20120j1u9nmkv534vw9vNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Sketchup-Rhino Cheat SheetDocument1 pageSketchup-Rhino Cheat Sheetxanext7No ratings yet
- Efficient Rice Based Cropping SystemDocument24 pagesEfficient Rice Based Cropping Systemsenthilnathan100% (1)
- Simple Roll-Type: A Loud SpeakerDocument1 pageSimple Roll-Type: A Loud SpeakerEudes SilvaNo ratings yet
- Relationsh Between EM and Young S ModuliDocument7 pagesRelationsh Between EM and Young S ModuliDwight AndersonNo ratings yet
- The Variable Resistor Has Been AdjustedDocument3 pagesThe Variable Resistor Has Been AdjustedPank O RamaNo ratings yet
- Uji Efektivitas Mikroba Rumpun BambuDocument7 pagesUji Efektivitas Mikroba Rumpun BambuUse Real ProjectNo ratings yet
- Aluminium Alloy - Wikipedia, The Free EncyclopediaDocument12 pagesAluminium Alloy - Wikipedia, The Free EncyclopediaAshishJoshi100% (1)
- Conformational Analysis: Carey & Sundberg: Part A Chapter 3Document53 pagesConformational Analysis: Carey & Sundberg: Part A Chapter 3Dr-Dinesh Kumar100% (1)
- Crashing Is A Schedule Compression Technique Used To Reduce or Shorten The Project ScheduleDocument1 pageCrashing Is A Schedule Compression Technique Used To Reduce or Shorten The Project ScheduleRaymart BulagsacNo ratings yet
- BECO UACE Chem2Document6 pagesBECO UACE Chem2EMMANUEL BIRUNGINo ratings yet
- Overall Method StatementDocument33 pagesOverall Method Statementsaranga100% (1)
- Full Download Short Term Financial Management 3rd Edition Maness Test BankDocument35 pagesFull Download Short Term Financial Management 3rd Edition Maness Test Bankcimanfavoriw100% (31)
- 7 +Royal+Court+Affairs,+Sultanate+of+OmanDocument12 pages7 +Royal+Court+Affairs,+Sultanate+of+OmanElencheliyan PandeeyanNo ratings yet
- Clinical Case StudyDocument20 pagesClinical Case Studyapi-252004748No ratings yet
- Five Star Hotel and ResortDocument9 pagesFive Star Hotel and ResortAISHNo ratings yet
- Predictive Maintenance Attempts To Detect The Onset of A Degradation Mechanism With The Goal of Correcting That Degradation Prior To Signiicant Deterioration in The Component or EquipmentDocument6 pagesPredictive Maintenance Attempts To Detect The Onset of A Degradation Mechanism With The Goal of Correcting That Degradation Prior To Signiicant Deterioration in The Component or EquipmentTodd BenjaminNo ratings yet
- ELIDA Products CatalogueDocument37 pagesELIDA Products CatalogueAbhishek AgarwalNo ratings yet
- Apcotide 1000 pc2782Document1 pageApcotide 1000 pc2782hellmanyaNo ratings yet
- Igcse Revision BookDocument23 pagesIgcse Revision BookJo Patrick100% (2)
- Multiple Choice Enzymes Plant and Animal NutritionDocument44 pagesMultiple Choice Enzymes Plant and Animal Nutritionliufanjing07No ratings yet
- Maths All FormulasDocument5 pagesMaths All FormulasVishnuNo ratings yet
- Tsel Manual ThermoselDocument25 pagesTsel Manual ThermoselPedro AlvelaisNo ratings yet
- Chemistry Notes: SUBJECT: Leaving Cert Chemistry Level: TEACHER: Tara LyonsDocument5 pagesChemistry Notes: SUBJECT: Leaving Cert Chemistry Level: TEACHER: Tara LyonsSevinc NuriyevaNo ratings yet
- Approved Project 25 StandardsDocument5 pagesApproved Project 25 StandardsepidavriosNo ratings yet
- Kodak Easyshare Z712 Is Zoom Digital Camera: User'S GuideDocument75 pagesKodak Easyshare Z712 Is Zoom Digital Camera: User'S GuideIronko PepeNo ratings yet
- Product Stock Exchange Learn BookDocument1 pageProduct Stock Exchange Learn BookSujit MauryaNo ratings yet
- Analysis of LaminatedDocument31 pagesAnalysis of LaminatedKaustubh JadhavNo ratings yet
- L2 Biostatistics ProbabilityDocument84 pagesL2 Biostatistics ProbabilityAaron CiudadNo ratings yet
- Spectroscopy (L-26 To 29)Document81 pagesSpectroscopy (L-26 To 29)Vashistha GargNo ratings yet