You might also like
- Borer (2013) Advanced Exercise Endocrinology PDFDocument272 pagesBorer (2013) Advanced Exercise Endocrinology PDFNicolás Bastarrica100% (1)
- Care of Mother, Child, Adolescent (Autosaved)Document23 pagesCare of Mother, Child, Adolescent (Autosaved)Shing Mae Marie100% (10)
- LAW OF ContractDocument1 pageLAW OF ContractKhurshid Manzoor Malik50% (2)
- Project Proposal On Child Nutrition For Sustainable Health and Prenatal ClinicDocument6 pagesProject Proposal On Child Nutrition For Sustainable Health and Prenatal Clinicczeremar chan100% (2)
- Changing Trends in Paediatric NursingDocument25 pagesChanging Trends in Paediatric NursingGayatri Mudliyar71% (7)
- Issues of Maternal and Child HealthDocument10 pagesIssues of Maternal and Child Healthjeelani saima100% (2)
- Care - of - Mother - Child - and - Adolescent 2Document48 pagesCare - of - Mother - Child - and - Adolescent 2Jmarie Brillantes PopiocoNo ratings yet
- Chapter01 A Framework For Maternal and Child NursingDocument36 pagesChapter01 A Framework For Maternal and Child NursingJoebeth Competente100% (1)
- 1.maternal and Child Health NursingDocument33 pages1.maternal and Child Health NursingBhie Bhie100% (1)
- Framework For MCHNDocument18 pagesFramework For MCHNchicklet escalonaNo ratings yet
- Notes - MCHN - Chapter 1Document12 pagesNotes - MCHN - Chapter 1Jamaica mitalNo ratings yet
- Frameworks MCHNDocument33 pagesFrameworks MCHNJerald FernandezNo ratings yet
- NCM 107 1st LectureDocument61 pagesNCM 107 1st LectureLyndon SulitNo ratings yet
- N-315: Family Health Nursing: Course Coordinator & Instructor: Mrs. Deepa ThomasDocument54 pagesN-315: Family Health Nursing: Course Coordinator & Instructor: Mrs. Deepa ThomasDeepa ThomasNo ratings yet
- Family HealthDocument23 pagesFamily HealthHassan Kafi AliNo ratings yet
- Maternal and Child NotesDocument26 pagesMaternal and Child NotesJann ericka JaoNo ratings yet
- Framework For Maternal and Child Health NursingDocument18 pagesFramework For Maternal and Child Health NursingTrisha ApalisNo ratings yet
- Week 1 NCM 107Document25 pagesWeek 1 NCM 107raise concern100% (1)
- Role of Nurse in Womens Health Trends, IssuesDocument27 pagesRole of Nurse in Womens Health Trends, Issuesalmayasa2002No ratings yet
- Module 1 Framework For Maternal and Child Health NursingDocument7 pagesModule 1 Framework For Maternal and Child Health NursingCha SahiddanNo ratings yet
- Module 1 MCNDocument5 pagesModule 1 MCNCha SahiddanNo ratings yet
- Obg Sem by Padmashree Institute of NursingDocument26 pagesObg Sem by Padmashree Institute of NursingmOHAN.S100% (1)
- Phases of Health CareDocument10 pagesPhases of Health Carecoosa liquors100% (1)
- Course Learning OutcomeDocument9 pagesCourse Learning OutcomeJumamoy, Bea ArabelaNo ratings yet
- Unit 5Document95 pagesUnit 5Sona amoreux De JESUSNo ratings yet
- NCM 109N: Frameworks For Maternal & Child Health NursingDocument37 pagesNCM 109N: Frameworks For Maternal & Child Health NursingZudota100% (1)
- LESSON 1.1 Maternal AND CHILDDocument11 pagesLESSON 1.1 Maternal AND CHILDAbegail Dapulag AdrayanNo ratings yet
- Ncm107mch Module1 FrameworkDocument30 pagesNcm107mch Module1 FrameworkVenus Anne LamayoNo ratings yet
- NCM 109 Lesson 1Document11 pagesNCM 109 Lesson 1eirelav0902No ratings yet
- Module 1 Framework For Maternal and Child NursingDocument2 pagesModule 1 Framework For Maternal and Child NursingJustine FloresNo ratings yet
- Health Care Programs - DOHDocument46 pagesHealth Care Programs - DOHZarlyn MirafloresNo ratings yet
- Family & Health Services SupportDocument42 pagesFamily & Health Services SupportYanti Efendy100% (2)
- 1 - Perspective of Child HealthDocument29 pages1 - Perspective of Child Healthamosae909No ratings yet
- Unit 1A.107 IntroductionDocument47 pagesUnit 1A.107 IntroductionHerbert EstremosNo ratings yet
- Maternal and Child Health Nursing Is Family-Centered Assessment DataDocument5 pagesMaternal and Child Health Nursing Is Family-Centered Assessment DataWendell Gian GolezNo ratings yet
- Maternal & Child Health CareDocument51 pagesMaternal & Child Health CareBhumi ChouhanNo ratings yet
- Maternal and Child Health NursingDocument1 pageMaternal and Child Health NursinggreinabelNo ratings yet
- Epidemiological Aspects of Maternal and Child Health and Its Issues Word ContentDocument40 pagesEpidemiological Aspects of Maternal and Child Health and Its Issues Word ContentNimi Simon100% (2)
- MCN 3Document32 pagesMCN 3Rainy Days100% (1)
- Unit 1A.107 IntroductionDocument56 pagesUnit 1A.107 Introductionma.jassein.oppus.21No ratings yet
- Chapter 1. A Framework For Maternal and Child Health NursingDocument11 pagesChapter 1. A Framework For Maternal and Child Health NursingAlyssaGrandeMontimorNo ratings yet
- Local Media958922746168865631Document8 pagesLocal Media958922746168865631Kate Lawrence BitantosNo ratings yet
- Pediatric Nursing 1الجزء الأولDocument291 pagesPediatric Nursing 1الجزء الأولVin Lorenzo CampbellNo ratings yet
- Pagcaliwagan, Beverly D. Bsn-Ii: Current Trends On Maternal and Child NursingDocument7 pagesPagcaliwagan, Beverly D. Bsn-Ii: Current Trends On Maternal and Child NursingBeverly PagcaliwaganNo ratings yet
- Maternal Nutritional AssessmentDocument7 pagesMaternal Nutritional AssessmentchinchuNo ratings yet
- Care of Mother, Child, AdolescentDocument18 pagesCare of Mother, Child, AdolescentShing Mae MarieNo ratings yet
- PRELIM CHN LECTURE HandoutsDocument22 pagesPRELIM CHN LECTURE HandoutsJOYCE ANN PEREGRINONo ratings yet
- Maternal and Child HealthDocument60 pagesMaternal and Child HealthStar AcademyNo ratings yet
- Mother Child HealthDocument62 pagesMother Child HealthTauseef AhmadNo ratings yet
- Notes On Maternal and Child Health NursingDocument3 pagesNotes On Maternal and Child Health NursingErika Bea PaculanangNo ratings yet
- MCH Report.. (Repaired)Document16 pagesMCH Report.. (Repaired)nathsujitkr1980No ratings yet
- Pediatrics Reviewer MCNDocument17 pagesPediatrics Reviewer MCNBrylee CudalNo ratings yet
- Epidemiological Aspects of Maternaland Child HealthDocument42 pagesEpidemiological Aspects of Maternaland Child HealthSusmita SenNo ratings yet
- Family Health ProgramsDocument58 pagesFamily Health ProgramsJabelle Mae DoteNo ratings yet
- Developmental TheoryDocument59 pagesDevelopmental Theorypramila subediNo ratings yet
- Chapter 1-3 ThesisDocument20 pagesChapter 1-3 ThesisMarianne Gonzales100% (1)
- Dona 1 CmcaDocument29 pagesDona 1 CmcaKyra MercadoNo ratings yet
- A Framework For Maternal and Child Health Nursing Care NCM 107Document3 pagesA Framework For Maternal and Child Health Nursing Care NCM 107Kyle VargasNo ratings yet
- OB-WORD (FRamework of Maternal Nursing)Document21 pagesOB-WORD (FRamework of Maternal Nursing)Danna MendozaNo ratings yet
- Rethinking Nutrition: Connecting Science and Practice in Early Childhood SettingsFrom EverandRethinking Nutrition: Connecting Science and Practice in Early Childhood SettingsNo ratings yet
- Family Nutrition GuideFrom EverandFamily Nutrition GuideNo ratings yet
- The Postnatal Cookbook: Simple and Nutritious Recipes to Nourish Your Body and Spirit During the Fourth TrimesterFrom EverandThe Postnatal Cookbook: Simple and Nutritious Recipes to Nourish Your Body and Spirit During the Fourth TrimesterNo ratings yet
- Hand WashingDocument1 pageHand WashingLawrence NemirNo ratings yet
- Non Traditional Nursing EducationDocument9 pagesNon Traditional Nursing EducationLawrence NemirNo ratings yet
- Gregorio A.Obra JR.: Head CookDocument2 pagesGregorio A.Obra JR.: Head CookLawrence NemirNo ratings yet
- Florence Nightingale ,: NursingDocument3 pagesFlorence Nightingale ,: NursingLawrence NemirNo ratings yet
- PharmacologyDocument11 pagesPharmacologyLawrence NemirNo ratings yet
- The Digestive System-FulDetailsEditedDocument28 pagesThe Digestive System-FulDetailsEditedLawrence NemirNo ratings yet
- Paniqui Backyard Gamecock Breeders Associatio2Document2 pagesPaniqui Backyard Gamecock Breeders Associatio2Lawrence NemirNo ratings yet
- Principles in Preparing For A Home A VisitDocument14 pagesPrinciples in Preparing For A Home A VisitLawrence NemirNo ratings yet
- Blood SugarDocument4 pagesBlood SugarLawrence NemirNo ratings yet
- PlanningDocument1 pagePlanningLawrence NemirNo ratings yet
- Structure of The Nervous SystemDocument2 pagesStructure of The Nervous SystemLawrence NemirNo ratings yet
- Circulatory Changes at BirthDocument3 pagesCirculatory Changes at BirthLawrence NemirNo ratings yet
- Circulatory Changes at BirthDocument3 pagesCirculatory Changes at BirthLawrence NemirNo ratings yet
- OrganizationDocument1 pageOrganizationLawrence NemirNo ratings yet
- Paniqui Backyard Gamecock Breeders AssociationDocument1 pagePaniqui Backyard Gamecock Breeders AssociationLawrence NemirNo ratings yet
- Michael B. Nemir RN, CRN, MSN: Good DayDocument1 pageMichael B. Nemir RN, CRN, MSN: Good DayLawrence NemirNo ratings yet
- Abnormal OBDocument34 pagesAbnormal OBLawrence NemirNo ratings yet
- Impact of Very Low Birth Weight On IQ and School PerformanceDocument1 pageImpact of Very Low Birth Weight On IQ and School PerformanceLawrence NemirNo ratings yet
- Generic NameDocument7 pagesGeneric NameLawrence NemirNo ratings yet
- Lawrence B. Nemir: BSN Iv-ADocument1 pageLawrence B. Nemir: BSN Iv-ALawrence NemirNo ratings yet
- Abnormal OBDocument34 pagesAbnormal OBLawrence NemirNo ratings yet
- Integrated Management of Childhood IllnessDocument2 pagesIntegrated Management of Childhood IllnessLawrence NemirNo ratings yet
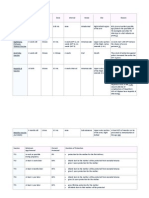
- Vaccine Minimum Age at 1st Dose Doses Dose Interval Route Site ReasonDocument2 pagesVaccine Minimum Age at 1st Dose Doses Dose Interval Route Site ReasonLawrence NemirNo ratings yet
- Cognitive DisordersDocument2 pagesCognitive DisordersSherrizah Alexis Naag NavaNo ratings yet
- Renal Parenchymal Disease T/C Acid Peptic DiseaseDocument43 pagesRenal Parenchymal Disease T/C Acid Peptic DiseaseLawrence NemirNo ratings yet
- PhysicsDocument8 pagesPhysicsLawrence NemirNo ratings yet
- PEG Catalog Siemens PDFDocument419 pagesPEG Catalog Siemens PDFrukmagoudNo ratings yet
- Economies of Scale in European Manufacturing Revisited: July 2001Document31 pagesEconomies of Scale in European Manufacturing Revisited: July 2001vladut_stan_5No ratings yet
- Applied Thermodynamics - DraughtDocument22 pagesApplied Thermodynamics - Draughtpiyush palNo ratings yet
- Charles P. Jones, Investments: Analysis and Management, Eleventh Edition, John Wiley & SonsDocument20 pagesCharles P. Jones, Investments: Analysis and Management, Eleventh Edition, John Wiley & SonsRizki AuliaNo ratings yet
- CrisisDocument13 pagesCrisisAngel Gaddi LarenaNo ratings yet
- InnovationDocument19 pagesInnovationPamela PlamenovaNo ratings yet
- Flabbergasted! - Core RulebookDocument160 pagesFlabbergasted! - Core RulebookRobert RichesonNo ratings yet
- 23 East 4Th Street NEW YORK, NY 10003 Orchard Enterprises Ny, IncDocument2 pages23 East 4Th Street NEW YORK, NY 10003 Orchard Enterprises Ny, IncPamelaNo ratings yet
- Espn NFL 2k5Document41 pagesEspn NFL 2k5jojojojo231No ratings yet
- MSC in Healthcare Management (Top-Up) Degree From ARU - Delivered Online by LSBR, UKDocument19 pagesMSC in Healthcare Management (Top-Up) Degree From ARU - Delivered Online by LSBR, UKLSBRNo ratings yet
- An Etymological Dictionary of The Scottivol 2Document737 pagesAn Etymological Dictionary of The Scottivol 2vstrohmeNo ratings yet
- KalamDocument8 pagesKalamRohitKumarSahuNo ratings yet
- Principles of Communication PlanDocument2 pagesPrinciples of Communication PlanRev Richmon De ChavezNo ratings yet
- Debarchana TrainingDocument45 pagesDebarchana TrainingNitin TibrewalNo ratings yet
- Government College of Engineering Jalgaon (M.S) : Examination Form (Approved)Document2 pagesGovernment College of Engineering Jalgaon (M.S) : Examination Form (Approved)Sachin Yadorao BisenNo ratings yet
- TN Vision 2023 PDFDocument68 pagesTN Vision 2023 PDFRajanbabu100% (1)
- Volvo D16 Engine Family: SpecificationsDocument3 pagesVolvo D16 Engine Family: SpecificationsJicheng PiaoNo ratings yet
- 15.597 B CAT en AccessoriesDocument60 pages15.597 B CAT en AccessoriesMohamed Choukri Azzoula100% (1)
- AnnulmentDocument9 pagesAnnulmentHumility Mae FrioNo ratings yet
- L 1 One On A Page PDFDocument128 pagesL 1 One On A Page PDFNana Kwame Osei AsareNo ratings yet
- Imogen Powerpoint DesignDocument29 pagesImogen Powerpoint DesignArthur100% (1)
- 1 Introduction To PPSTDocument52 pages1 Introduction To PPSTpanabo central elem sch.No ratings yet
- Discrete Probability Distribution UpdatedDocument44 pagesDiscrete Probability Distribution UpdatedWaylonNo ratings yet
- Rebecca Young Vs CADocument3 pagesRebecca Young Vs CAJay RibsNo ratings yet
- Custom Belt Buckles: Custom Brass Belt Buckles - Hand Made in The USA - Lifetime Guarantee of QualityDocument1 pageCustom Belt Buckles: Custom Brass Belt Buckles - Hand Made in The USA - Lifetime Guarantee of QualityAndrew HunterNo ratings yet
- Army Public School Recruitment 2017Document9 pagesArmy Public School Recruitment 2017Hiten BansalNo ratings yet
- Multi Grade-ReportDocument19 pagesMulti Grade-Reportjoy pamorNo ratings yet
- Performance MeasurementDocument13 pagesPerformance MeasurementAmara PrabasariNo ratings yet