You might also like
- TÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANOFrom EverandTÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANONo ratings yet
- Turn Around Time.30901815Document6 pagesTurn Around Time.30901815Divya Shetty100% (1)
- Medical Integration Model as it Pertains to Musculoskeletal ConditionsFrom EverandMedical Integration Model as it Pertains to Musculoskeletal ConditionsNo ratings yet
- Discharge PlanningDocument5 pagesDischarge PlanningPujiNo ratings yet
- Handbook for Cssd Technicians: Understanding the Basics - Second EditionFrom EverandHandbook for Cssd Technicians: Understanding the Basics - Second EditionNo ratings yet
- CIrurgia Anestesia Start TimeDocument4 pagesCIrurgia Anestesia Start TimethannasNo ratings yet
- Problem2013 PDFDocument6 pagesProblem2013 PDFEscuela Industriales UPMNo ratings yet
- Orthopeadic ClinicDocument6 pagesOrthopeadic ClinicGemini_0804100% (3)
- Qsir Discharge PlanningDocument5 pagesQsir Discharge Planningmargaret kuuNo ratings yet
- Value Stream MappingDocument16 pagesValue Stream MappingOINDRILA KARMAKAR06100% (2)
- Admitting Patient: When Admitting A Patient What Are The Basic Procedures?Document4 pagesAdmitting Patient: When Admitting A Patient What Are The Basic Procedures?diah ayuNo ratings yet
- Articulo CientificoDocument12 pagesArticulo CientificoAngeles Jiménez DuhartNo ratings yet
- 2010 Seven Ways To No Delays FINAL (Low-Res)Document24 pages2010 Seven Ways To No Delays FINAL (Low-Res)Ruby SharmaNo ratings yet
- Modeling Interruptions and Patient Flow in A Preoperative Hospital EnvironmentDocument11 pagesModeling Interruptions and Patient Flow in A Preoperative Hospital EnvironmentLuruh Bersama HujanNo ratings yet
- Journal Pre-Proof: Journal of Plastic, Reconstructive & Aesthetic SurgeryDocument10 pagesJournal Pre-Proof: Journal of Plastic, Reconstructive & Aesthetic SurgeryMaitham IsmailNo ratings yet
- Aakash Patient Care Services AssingmentDocument10 pagesAakash Patient Care Services Assingmentaakash sharmaNo ratings yet
- Casestudy Analysis Template Updated 18 Oct 16Document2 pagesCasestudy Analysis Template Updated 18 Oct 16keven319hk4304No ratings yet
- Ots 24 Oac30-51 4annexurDocument22 pagesOts 24 Oac30-51 4annexurapi-3774915No ratings yet
- Hipkneejourneyguide Web 1Document32 pagesHipkneejourneyguide Web 1api-501409374No ratings yet
- A Day in The Life of An Orthopedic Rep A Real Life AccountDocument5 pagesA Day in The Life of An Orthopedic Rep A Real Life AccountLulu LsabNo ratings yet
- A Study On Process and Analysis of Opd Waiting Time in Phlebotomy AreaDocument29 pagesA Study On Process and Analysis of Opd Waiting Time in Phlebotomy AreaMiracle Online ServicesNo ratings yet
- SSRN Id3819868Document87 pagesSSRN Id3819868Chester Adriaan HendricksNo ratings yet
- Shouldice Hospital Group8Document8 pagesShouldice Hospital Group8Rahul Shankar0% (1)
- What's So Hard About Bronchoscopic Surgery?Document5 pagesWhat's So Hard About Bronchoscopic Surgery?Marc DijkstraNo ratings yet
- Surgerypaper June 6Document23 pagesSurgerypaper June 6Deepali KoiralaNo ratings yet
- POC CHWO HW Solutions PDFDocument5 pagesPOC CHWO HW Solutions PDFakashkr619No ratings yet
- Sirgut Tesfaye Simulation ProjectDocument19 pagesSirgut Tesfaye Simulation ProjectSirgut TesfayeNo ratings yet
- Kashulwe Report For WilDocument11 pagesKashulwe Report For WilJonathan LukwichiNo ratings yet
- Pre Op MNGMNTDocument22 pagesPre Op MNGMNTsandeepv08No ratings yet
- Reasons For Delay in Turnover Time in Operating Room An Observational Studybangladesh Journal of Medical ScienceDocument7 pagesReasons For Delay in Turnover Time in Operating Room An Observational Studybangladesh Journal of Medical ScienceKshitiz112No ratings yet
- Class Excercise - Session 2Document4 pagesClass Excercise - Session 2rahul prasadNo ratings yet
- Early Postoperative Ambulation Back To Basics A Quality Improvement Project PDFDocument7 pagesEarly Postoperative Ambulation Back To Basics A Quality Improvement Project PDFIndra MulianiNo ratings yet
- Reducing Waiting Time of Patients in Outpatient Services of Large Teaching Hospital: A Systematic Quality ApproachDocument7 pagesReducing Waiting Time of Patients in Outpatient Services of Large Teaching Hospital: A Systematic Quality ApproachRajni KumariNo ratings yet
- #Design and Implementation of Computerized Medical Duties Scheduling System - Inimax HubDocument77 pages#Design and Implementation of Computerized Medical Duties Scheduling System - Inimax HubclarusNo ratings yet
- Reducing Bed Turnover DelaysDocument4 pagesReducing Bed Turnover DelayskukunNo ratings yet
- Surgery Scheduling: Industrial Engineering TED UniversityDocument56 pagesSurgery Scheduling: Industrial Engineering TED UniversityMurat DenizNo ratings yet
- Six SigmaDocument4 pagesSix SigmaPrateik BhasinNo ratings yet
- Shouldice Hospital SolutionDocument8 pagesShouldice Hospital SolutionSyed Ahmer RizviNo ratings yet
- Admission DischargeDocument30 pagesAdmission Dischargedigracia manatigaNo ratings yet
- Assistant Workshop FinalDocument33 pagesAssistant Workshop FinalJay PuriNo ratings yet
- Applying Lean Techniques To Improve The Patient Scheduling ProcessDocument7 pagesApplying Lean Techniques To Improve The Patient Scheduling ProcessjessicaNo ratings yet
- MSCI 102 Coursework ReportDocument8 pagesMSCI 102 Coursework ReportMartin AndreevNo ratings yet
- OB TriageDocument36 pagesOB TriagerelinNo ratings yet
- Discharge Process SynopsisDocument7 pagesDischarge Process Synopsisdrbhavya250% (1)
- MGH PataDocument16 pagesMGH PataJireh Acabal86% (14)
- No. 27 PDFDocument7 pagesNo. 27 PDFAdilah Zatil KurniaNo ratings yet
- Internet Case For Supplement 7Document3 pagesInternet Case For Supplement 7johnmia20No ratings yet
- Relationshipbasedcarepaper - NSG 4040-1Document13 pagesRelationshipbasedcarepaper - NSG 4040-1api-314231356No ratings yet
- RNFA As ConciergeDocument13 pagesRNFA As ConciergeLisaNo ratings yet
- Team 1 Shouldice HospitalDocument15 pagesTeam 1 Shouldice HospitalRahul Shankar100% (3)
- Management 1 NotesDocument14 pagesManagement 1 NotesSteve OnyangoNo ratings yet
- Electronic Medical Handover: Towards Safer Medical CareDocument4 pagesElectronic Medical Handover: Towards Safer Medical CareLuminita StoleruNo ratings yet
- Case ShouldiceDocument3 pagesCase ShouldiceThắng ViếtNo ratings yet
- Shouldice Hospital CaseDocument4 pagesShouldice Hospital CaseRikiAchinta100% (1)
- Don't Lose PatientsDocument9 pagesDon't Lose PatientsdrustagiNo ratings yet
- A Hospital Unit Performance CalculatorDocument15 pagesA Hospital Unit Performance CalculatorloloNo ratings yet
- AssignmentDocument3 pagesAssignmentJam Sohail Ahmed DaharNo ratings yet
- Dayton Medical Care, Inc. (Day-Med) Patient Appointment SystemDocument4 pagesDayton Medical Care, Inc. (Day-Med) Patient Appointment SystemJoel Christian MascariñaNo ratings yet
- Proposal For Hospital System: EER Diagram & Relational ModelDocument11 pagesProposal For Hospital System: EER Diagram & Relational ModelAhmed Sh0% (1)
- A Case Study On Shouldice HospitalDocument34 pagesA Case Study On Shouldice HospitalSelwin DsouzaNo ratings yet
- The Business Vision and Mission: Chapter TwoDocument24 pagesThe Business Vision and Mission: Chapter Twofahadfiaz100% (1)
- SM Outline & Ch1Document44 pagesSM Outline & Ch1fahadfiazNo ratings yet
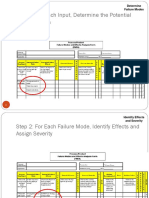
- Step 1: For Each Input, Determine The Potential Failure ModesDocument7 pagesStep 1: For Each Input, Determine The Potential Failure ModesfahadfiazNo ratings yet
- Bruce Henderson: Boston Consulting Group (BCG) MATRIX Is Developed by Consulting Group in The Early 1970'SDocument17 pagesBruce Henderson: Boston Consulting Group (BCG) MATRIX Is Developed by Consulting Group in The Early 1970'SfahadfiazNo ratings yet
- Pakistan Quality AwardDocument7 pagesPakistan Quality AwardfahadfiazNo ratings yet
- A Review of ISO 9000 ImpactDocument5 pagesA Review of ISO 9000 ImpactfahadfiazNo ratings yet
- QUestionnaire 001 003Document3 pagesQUestionnaire 001 003fahadfiazNo ratings yet
- WWW Qualityfoundation in Sqc7 Basic Qctools HTMLDocument14 pagesWWW Qualityfoundation in Sqc7 Basic Qctools HTMLfahadfiazNo ratings yet
- Career MGTDocument18 pagesCareer MGTfahadfiazNo ratings yet
- Control Engineering: Prepared By: Muhammad Moeen SultanDocument111 pagesControl Engineering: Prepared By: Muhammad Moeen SultanfahadfiazNo ratings yet
- Questionnaire On TQM Implementation PDFDocument8 pagesQuestionnaire On TQM Implementation PDFfahadfiaz100% (2)
- Experiment No.1: Now Manually Move The AVS-1 Bar To Control The Flow Through The Valve in To The ContainerDocument16 pagesExperiment No.1: Now Manually Move The AVS-1 Bar To Control The Flow Through The Valve in To The ContainerfahadfiazNo ratings yet
- B Jack Nos For Cs Ss MaterialDocument12 pagesB Jack Nos For Cs Ss MaterialfahadfiazNo ratings yet
- MATLAB ArraysDocument17 pagesMATLAB ArraysfahadfiazNo ratings yet
- Control Engineering: Prepared By: Muhammad Moeen SultanDocument34 pagesControl Engineering: Prepared By: Muhammad Moeen SultanfahadfiazNo ratings yet
- Vessel Allowable LoadingsDocument50 pagesVessel Allowable LoadingsfahadfiazNo ratings yet
- Computer Fundamentals-Lab manual-MATLABDocument6 pagesComputer Fundamentals-Lab manual-MATLABfahadfiazNo ratings yet
- Control Engineering: Prepared By: Muhammad Moeen SultanDocument36 pagesControl Engineering: Prepared By: Muhammad Moeen SultanfahadfiazNo ratings yet
- Control Engineering: Prepared By: Muhammad Moeen SultanDocument67 pagesControl Engineering: Prepared By: Muhammad Moeen SultanfahadfiazNo ratings yet
- MCQ Pead MockDocument8 pagesMCQ Pead MocknoblefxNo ratings yet
- AdenomyosisDocument1 pageAdenomyosisVictor GomoiuNo ratings yet
- Strength Training & Weight Training 101Document28 pagesStrength Training & Weight Training 101Maru PabloNo ratings yet
- Pharmacology Book - PharmaceuticsDocument48 pagesPharmacology Book - PharmaceuticsRuchi SinghNo ratings yet
- Antimalarials - Are They Effective and Safe in Rheumatic DiseasesDocument10 pagesAntimalarials - Are They Effective and Safe in Rheumatic DiseasesYahya RizkiNo ratings yet
- The - Utics and Control of Sheep and Goat Diseases, An Issue of Veterinary Clinics, Food Animal PracticeDocument262 pagesThe - Utics and Control of Sheep and Goat Diseases, An Issue of Veterinary Clinics, Food Animal PracticeIurydyana Villalobos0% (1)
- Stem Cell Research PaperDocument3 pagesStem Cell Research Papermyrentistoodamnhigh100% (1)
- AcetanilideDocument4 pagesAcetanilideJinseong ChoiNo ratings yet
- Lab Policies Differential Counting and Morphology Lab 5074Document14 pagesLab Policies Differential Counting and Morphology Lab 5074Egil SantosNo ratings yet
- Astm E446 ReqDocument3 pagesAstm E446 ReqwerwewmnlljlajkdNo ratings yet
- ICD X Kes HajiDocument2 pagesICD X Kes Hajiyasin_rsdk67% (3)
- Taema Monnal D2 Anaesthesia Machine - Users ManualDocument13 pagesTaema Monnal D2 Anaesthesia Machine - Users ManualJuan carlosNo ratings yet
- How Will The Coca-Cola Avoid The Big Loss For Launching A Wrong Product?Document4 pagesHow Will The Coca-Cola Avoid The Big Loss For Launching A Wrong Product?Ashwani Kumar SahuNo ratings yet
- PACS Basics PDFDocument6 pagesPACS Basics PDFBalaji BalasubramanianNo ratings yet
- HfiDocument4 pagesHfiakalaw3No ratings yet
- Intern Annual16Document7 pagesIntern Annual16Akash PanwarNo ratings yet
- CHP 11 Moderate Nonskeletal Problems in Preadolescent ChildrenDocument6 pagesCHP 11 Moderate Nonskeletal Problems in Preadolescent ChildrenJack Pai33% (3)
- Negatil Tablet: What Is in This LeafletDocument2 pagesNegatil Tablet: What Is in This LeafletEe JoNo ratings yet
- Quality Management in The Imaging Sciences 5th Edition Papp Test BankDocument35 pagesQuality Management in The Imaging Sciences 5th Edition Papp Test Bankmisdateholinessaubzt6100% (22)
- Schizophrenia Coursework - Jack Kerouac PresentationDocument16 pagesSchizophrenia Coursework - Jack Kerouac PresentationCMNo ratings yet
- DAFTAR PUSTAKA (Kasus Mendalam 2)Document4 pagesDAFTAR PUSTAKA (Kasus Mendalam 2)mkpnurdinNo ratings yet
- Uniformity of Dosage UnitsDocument5 pagesUniformity of Dosage UnitsJai MurugeshNo ratings yet
- B VCM 009501Document129 pagesB VCM 009501Evelyn Carolina Sepulveda CespedesNo ratings yet
- Roles and Responsibilities of ASHADocument3 pagesRoles and Responsibilities of ASHAmohanpskohli8310No ratings yet
- JMM 29 119Document8 pagesJMM 29 119subanant11No ratings yet
- Application Form (Pledge Form) For Whole Body DonationDocument1 pageApplication Form (Pledge Form) For Whole Body DonationVasanthakumar BasavaNo ratings yet
- Funda ConceptsDocument201 pagesFunda ConceptsEncee Mian0% (1)
- The Accidental AddictsDocument6 pagesThe Accidental AddictsnorthandsouthnzNo ratings yet
- Emr Policy and ProcedureDocument7 pagesEmr Policy and Procedureapi-267965870No ratings yet
- OHS-TBT-010 - Types of Hazards - 1Document1 pageOHS-TBT-010 - Types of Hazards - 1Tony NhabangaNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (33)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (82)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (4)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeRating: 4.5 out of 5 stars4.5/5 (2)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (254)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (60)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Hearts of Darkness: Serial Killers, The Behavioral Science Unit, and My Life as a Woman in the FBIFrom EverandHearts of Darkness: Serial Killers, The Behavioral Science Unit, and My Life as a Woman in the FBIRating: 4 out of 5 stars4/5 (20)