You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Bridge Course Mathematics 2022-23 - IxDocument21 pagesBridge Course Mathematics 2022-23 - IxManish RathoreNo ratings yet
- The Brook - Poetic DevicesDocument3 pagesThe Brook - Poetic Devicesraaj67% (12)
- Astm D5454 11 2020Document1 pageAstm D5454 11 2020MiguelNo ratings yet
- Chapter Three: Risk Indicators For Displaced Abomasum On Herd LevelDocument12 pagesChapter Three: Risk Indicators For Displaced Abomasum On Herd LevelfrankyNo ratings yet
- Applications Pumped Liquids: Agriculture Domestic Irrigation Gardens Industrial Rural Water SupplyDocument5 pagesApplications Pumped Liquids: Agriculture Domestic Irrigation Gardens Industrial Rural Water Supplyகோவி கோபால் ஆர்ட்ஸ்No ratings yet
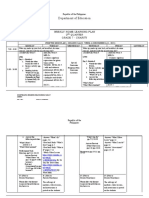
- Philippine Department of Education Home Learning Plan for Grade 7Document13 pagesPhilippine Department of Education Home Learning Plan for Grade 7Charlene AtienzaNo ratings yet
- Machine Design of Hoists, Derricks and Cranes by HessDocument440 pagesMachine Design of Hoists, Derricks and Cranes by HessDickson Leong67% (3)
- BT Cargo Compact Electric-749836-040Document58 pagesBT Cargo Compact Electric-749836-040chamithpNo ratings yet
- Mapeo ComputoDocument20 pagesMapeo ComputoGuillermo Santiago Robles RangelNo ratings yet
- Air Compressor Capacity and Air Reciever SizingDocument3 pagesAir Compressor Capacity and Air Reciever SizingHasmukh DaveNo ratings yet
- 200A, 15 KV Class Loadbreak Rotatable Feed Thru Insert: 15-LFTI200Document3 pages200A, 15 KV Class Loadbreak Rotatable Feed Thru Insert: 15-LFTI200Diego AlvesNo ratings yet
- SCC - Electonics - Q4M3Weeks5-6 - PASSED NO AKDocument18 pagesSCC - Electonics - Q4M3Weeks5-6 - PASSED NO AKLyle Isaac L. IllagaNo ratings yet
- his Life": Λογοτεχνία και διαπολιτισμικές διαδρομές Literature and cross‐cultural routesDocument18 pageshis Life": Λογοτεχνία και διαπολιτισμικές διαδρομές Literature and cross‐cultural routesCharpapathNo ratings yet
- Matter: Quarter 1: Module 5 - 7Document29 pagesMatter: Quarter 1: Module 5 - 7Aizy AlmosaraNo ratings yet
- 4024 w08 Ms 2Document9 pages4024 w08 Ms 2mstudy123456No ratings yet
- MKKL 2063Document10 pagesMKKL 2063Anas Abd RahmanNo ratings yet
- Cre Technology ParallelingDocument6 pagesCre Technology ParallelingduaNo ratings yet
- Solid State Phy-RPDocument39 pagesSolid State Phy-RPAbhijan Carter BiswasNo ratings yet
- PK Solutions 2.0 PK Solutions 2.0 PK Solutions 2.0 PK Solutions 2.0Document18 pagesPK Solutions 2.0 PK Solutions 2.0 PK Solutions 2.0 PK Solutions 2.0rigaut74No ratings yet
- Standard Test Method For Splitting Tensile Strength of Cylindrical Concrete Specimens1Document5 pagesStandard Test Method For Splitting Tensile Strength of Cylindrical Concrete Specimens1Lupita RamirezNo ratings yet
- Marcom Opc ProductsDocument8 pagesMarcom Opc ProductsMARCOM SRLNo ratings yet
- Hacking - 201204Document75 pagesHacking - 201204Danilo CarusoNo ratings yet
- Common Laboratory ProcedureDocument4 pagesCommon Laboratory Procedureripsky17No ratings yet
- Rubik Cube Solver ReportDocument11 pagesRubik Cube Solver ReportDarthstarNo ratings yet
- Woodworth (1899) The Accuracy of Voluntary MovementDocument120 pagesWoodworth (1899) The Accuracy of Voluntary MovementInacioRabaioli0% (2)
- Covid-19 and Crises Management Strategies of Hospitality Industry: A Descriptive ResearchDocument8 pagesCovid-19 and Crises Management Strategies of Hospitality Industry: A Descriptive ResearchIAEME PublicationNo ratings yet
- Wireless World 1983 10Document118 pagesWireless World 1983 10asd100% (1)
- Biochem 12th Sept Amino AcidDocument4 pagesBiochem 12th Sept Amino AcidShreeraj BadgujarNo ratings yet
- KPIs Subcounters 14apr15 V1-NOKBSC-SEG-hour-PM 10530-2018 04 15-15 49 41 855Document102 pagesKPIs Subcounters 14apr15 V1-NOKBSC-SEG-hour-PM 10530-2018 04 15-15 49 41 855AmMood GmrNo ratings yet
- Introduction To Java - DAY1Document16 pagesIntroduction To Java - DAY1anthims ZohoNo ratings yet