You might also like
- Handbook for Cssd Technicians: Understanding the Basics - Second EditionFrom EverandHandbook for Cssd Technicians: Understanding the Basics - Second EditionNo ratings yet
- The COAT & Review Approach: How to recognise and manage unwell patientsFrom EverandThe COAT & Review Approach: How to recognise and manage unwell patientsRating: 5 out of 5 stars5/5 (1)
- Clinical Casuality ManagementDocument6 pagesClinical Casuality ManagementswathiprasadNo ratings yet
- Toledo Code Blue PolicyDocument4 pagesToledo Code Blue PolicySt SNo ratings yet
- JCI Accreditation Presentation 4Document53 pagesJCI Accreditation Presentation 4Osama MarzoukNo ratings yet
- MedicineDocument19 pagesMedicineSarah100% (1)
- prehospital-EMS-COVID-19-recommendations - 4.4Document19 pagesprehospital-EMS-COVID-19-recommendations - 4.4MEONENo ratings yet
- Emergency Departement in Aiyiyah Mother and Child HospitalDocument3 pagesEmergency Departement in Aiyiyah Mother and Child HospitalHida Tri NurrochmahNo ratings yet
- Assignment ON Documentation: Submitted To: Submitted byDocument12 pagesAssignment ON Documentation: Submitted To: Submitted byNagulan Nagul100% (1)
- 17 Admission APP MED 001Document8 pages17 Admission APP MED 001HAMMYER ALROKHAMINo ratings yet
- Procedure Manual HospitalDocument196 pagesProcedure Manual HospitalMarian StrihaNo ratings yet
- Arero Primary Hospital Triage ProtocolDocument4 pagesArero Primary Hospital Triage Protocolsami ketemaNo ratings yet
- GOI Draft-SOPs-for-Hospital-managementDocument38 pagesGOI Draft-SOPs-for-Hospital-managementksushruuthNo ratings yet
- Inter Hospital Transfer SopDocument2 pagesInter Hospital Transfer SopNATARAJAN RAJENDRANNo ratings yet
- Ed Assessment Tool SampleDocument28 pagesEd Assessment Tool SampleAnonymous ibmeej9No ratings yet
- 1.1 Hospital Fire PlanDocument8 pages1.1 Hospital Fire Planjcspai100% (2)
- Case Study - Lilavati: HospitalDocument39 pagesCase Study - Lilavati: HospitalCharanjeet Singh AroraNo ratings yet
- COP 3 & PFR 1.5 - Care of Vulnerable PatientsDocument4 pagesCOP 3 & PFR 1.5 - Care of Vulnerable Patientsn_robinNo ratings yet
- Missing Patients ProcedureDocument16 pagesMissing Patients ProcedureAgnieszka WaligóraNo ratings yet
- Hospital Disaster Management Plan - Draft1-MkDocument71 pagesHospital Disaster Management Plan - Draft1-MkAdri FitriNo ratings yet
- 2011 Newborn Care SOP 29-11-11Document95 pages2011 Newborn Care SOP 29-11-11Safiqul Islam ShawnNo ratings yet
- Nurse Bob's MICU/CCU Survival Guide Critical Care Concepts General Nursing Requirements of The Intensive Care PatientDocument7 pagesNurse Bob's MICU/CCU Survival Guide Critical Care Concepts General Nursing Requirements of The Intensive Care Patientlil' princessNo ratings yet
- Hospital Emergency Management PlanDocument5 pagesHospital Emergency Management PlandedefreddyNo ratings yet
- Admitting A Patient .: Prepared by Ayugi Winnyfred Patience Bsc. Midwifery StudentDocument10 pagesAdmitting A Patient .: Prepared by Ayugi Winnyfred Patience Bsc. Midwifery StudentAYO NELSONNo ratings yet
- Accident and EmergenciesDocument5 pagesAccident and EmergenciesArnel AlmutiahNo ratings yet
- Preoperative Assessment PolicyDocument10 pagesPreoperative Assessment PolicymandayogNo ratings yet
- CLCGP030 Theatre Operating List Session Scheduling PolicyDocument19 pagesCLCGP030 Theatre Operating List Session Scheduling PolicyJeffy PuruggananNo ratings yet
- 3a - Occupational Safety ME 70 Basic Occupational Safety and HealthDocument91 pages3a - Occupational Safety ME 70 Basic Occupational Safety and Healths.salise.allendaveNo ratings yet
- Clinical Establishment Act Standards For Hospital (LEVEL 3)Document36 pagesClinical Establishment Act Standards For Hospital (LEVEL 3)bksubrat100% (3)
- IPD SOP DraftDocument13 pagesIPD SOP DraftvvvvtusebtNo ratings yet
- TRIAGE POLICIES JuvyDocument6 pagesTRIAGE POLICIES JuvyCuyapo Infirmary Lying-In HospitalNo ratings yet
- Nursing Audit Tool PDFDocument12 pagesNursing Audit Tool PDFjamieNo ratings yet
- Western Australian Patient Identification Policy PDFDocument14 pagesWestern Australian Patient Identification Policy PDFpuspadiniaNo ratings yet
- In - Patient Service Ward 1Document12 pagesIn - Patient Service Ward 1mitchNo ratings yet
- Accident and Emergency DepartmentDocument9 pagesAccident and Emergency Departmentshah007zaadNo ratings yet
- Kpi Wards 2021 - A WingDocument48 pagesKpi Wards 2021 - A WingPriya LaddhaNo ratings yet
- Emergency NursingDocument15 pagesEmergency NursingAshley Ishika100% (1)
- CHA Hospital Activation of The Emergency Operations Plan ChecklistDocument5 pagesCHA Hospital Activation of The Emergency Operations Plan Checklistraysub159No ratings yet
- Annual Plan: Infection Prevention & Control DepartmentDocument3 pagesAnnual Plan: Infection Prevention & Control DepartmentSherina Edding0% (1)
- Job Responsibilities FoDocument4 pagesJob Responsibilities FoKumar BalramNo ratings yet
- Emergency Department Operational SOP v1.1 Mar2017Document15 pagesEmergency Department Operational SOP v1.1 Mar2017agelesswapNo ratings yet
- Inpatient DepartmentDocument7 pagesInpatient Departmentshah007zaadNo ratings yet
- Standardized Emergency Color CodesDocument1 pageStandardized Emergency Color CodesDivya ToppoNo ratings yet
- How To Move The Patient From The Bed To The Wheelchair How To Move The Patient From The Bed To The WheelchairDocument9 pagesHow To Move The Patient From The Bed To The Wheelchair How To Move The Patient From The Bed To The WheelchairAfniy ApriliaNo ratings yet
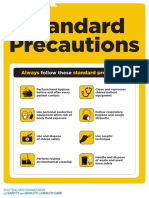
- Approach 4 Standard Precautions Icon PDF 672KBDocument1 pageApproach 4 Standard Precautions Icon PDF 672KBElaine MacalandaNo ratings yet
- Monitoring Tool For Evluation of Performance of The Staff Nurse During Admission, Transfer & Discharge of The PatientDocument12 pagesMonitoring Tool For Evluation of Performance of The Staff Nurse During Admission, Transfer & Discharge of The Patientmahbuburrahim9553No ratings yet
- 4503 Nursing Credentialing ProcedureDocument6 pages4503 Nursing Credentialing Procedurereve777No ratings yet
- Report On HIRA in Fortis Hospital AmritsarDocument15 pagesReport On HIRA in Fortis Hospital AmritsarUmar LoneNo ratings yet
- Central Triage ProtocolDocument1 pageCentral Triage Protocolgechworkneh38No ratings yet
- Fire Safety QuestionsDocument3 pagesFire Safety Questionsbalaji srinivasanNo ratings yet
- Code NurseDocument2 pagesCode Nursenoreen ellie100% (2)
- SOP - CQI ProgramDocument20 pagesSOP - CQI Programaaminah tariqNo ratings yet
- List of Hospital Committees and Teams For NABH Accreditation PreparationDocument6 pagesList of Hospital Committees and Teams For NABH Accreditation PreparationSanjay KadamNo ratings yet
- 724 - Admissions Policy Procedure and Guidelines PDFDocument106 pages724 - Admissions Policy Procedure and Guidelines PDFSonyKurniawanNo ratings yet
- Intensive Care UnitDocument12 pagesIntensive Care UnitAnt OnNo ratings yet
- Checklist of Anaesthesia Department For NABH Accreditation PreparationDocument3 pagesChecklist of Anaesthesia Department For NABH Accreditation PreparationPayal ThakkerNo ratings yet
- 31-Nursing Assessment For Out Patient DepartmentDocument2 pages31-Nursing Assessment For Out Patient DepartmentakositabonNo ratings yet
- UNIT-1: Essentials of E-Commerce & HTMLDocument125 pagesUNIT-1: Essentials of E-Commerce & HTMLmanisha GuptaNo ratings yet
- Nursing Services Manual, Aiims New Delhi - 25!2!21Document91 pagesNursing Services Manual, Aiims New Delhi - 25!2!21praveenjenaNo ratings yet
- Errors in NursingDocument59 pagesErrors in NursingCzerwin JualesNo ratings yet
- 5000 Nik Dan KK (Sfile PDFDocument44 pages5000 Nik Dan KK (Sfile PDFGhina Sakila100% (1)
- MicrologDocument1 pageMicrologmursidahanimNo ratings yet
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Chapter 6 Water Safety - Recognition and ResponseDocument41 pagesChapter 6 Water Safety - Recognition and ResponsemaligayamicadaleNo ratings yet
- Chapter 5 - Understanding Evidence-Based PracticeDocument29 pagesChapter 5 - Understanding Evidence-Based PracticeIgnacio TroianoNo ratings yet
- EULAR Recommendations For Prevention and Management of Osteoporotic FracturesDocument9 pagesEULAR Recommendations For Prevention and Management of Osteoporotic FracturesTurboNo ratings yet
- Walsh2015association of Diabetic Foot Ulcer and Death in A Population-Based Cohort From The United KingdomDocument6 pagesWalsh2015association of Diabetic Foot Ulcer and Death in A Population-Based Cohort From The United KingdomAnonymous SMLzNANo ratings yet
- Medical Surgical NursingDocument110 pagesMedical Surgical Nursingarjetahoward100% (5)
- Gavage Feeding RepDocument6 pagesGavage Feeding RepEon Provido AlfaroNo ratings yet
- BTL-Aesthetics ED AE-guide-supplement EN100Document8 pagesBTL-Aesthetics ED AE-guide-supplement EN100joaquina.espinoza20No ratings yet
- Advanced Practice RolesDocument16 pagesAdvanced Practice RolesLorelie Asis0% (1)
- FARMASAINS Vol. Xx. No. XX, Bulan TahunDocument9 pagesFARMASAINS Vol. Xx. No. XX, Bulan TahunShonia FatwaNo ratings yet
- Warfarin Reversal Guideline 2012 PDFDocument8 pagesWarfarin Reversal Guideline 2012 PDFVlady78No ratings yet
- ACNS Standardized Critical Care EEG Examples 2021Document36 pagesACNS Standardized Critical Care EEG Examples 2021CNo ratings yet
- Journal of Interventional Medicine: Yanli Wang, Guohao Huang, Tian Jiang, Xinwei HanDocument5 pagesJournal of Interventional Medicine: Yanli Wang, Guohao Huang, Tian Jiang, Xinwei HanDzulRizkaNo ratings yet
- DISSociative AnaesthesiaDocument3 pagesDISSociative Anaesthesiamohit jainNo ratings yet
- Types of Body Conditioning Exercises: and Their BenefitsDocument32 pagesTypes of Body Conditioning Exercises: and Their Benefitscrizel in nameNo ratings yet
- Caesarean SectionDocument23 pagesCaesarean SectionIdiAmadouNo ratings yet
- H5N1 EngDocument8 pagesH5N1 EngHường ĐỗNo ratings yet
- Recommendations CardiovascularRenal 07.09.2022Document6 pagesRecommendations CardiovascularRenal 07.09.2022Harisankarthekkethil 26No ratings yet
- Heart With 67 StentsDocument3 pagesHeart With 67 StentstomriedmanNo ratings yet
- Grave's Ophthalmopathy: Susy Fatmariyanti Delfitri Lutfi, Hendrian D. SoebagjoDocument12 pagesGrave's Ophthalmopathy: Susy Fatmariyanti Delfitri Lutfi, Hendrian D. SoebagjoriskhapangestikaNo ratings yet
- Med-Surg Lecture 4th Year 1st Sem (Incomplete)Document70 pagesMed-Surg Lecture 4th Year 1st Sem (Incomplete)Raezhell Dianne RachoNo ratings yet
- Kit Insert HDL Bahasa IndonesiaDocument2 pagesKit Insert HDL Bahasa IndonesiaAhraNo ratings yet
- Brown (2001) PDFDocument13 pagesBrown (2001) PDFAna Catarina InácioNo ratings yet
- Arthur Steindler: Pes Cavus (1921), He Analyzed The Muscle ImbalDocument3 pagesArthur Steindler: Pes Cavus (1921), He Analyzed The Muscle Imbalisaac b-127No ratings yet
- Jurnal ReadingDocument22 pagesJurnal Readingarismaputra20No ratings yet
- The Prevalence of Depression and Anxiety in Iranian Patients With Diabetes Mellitus: A Systematic Review and Meta-AnalysisDocument11 pagesThe Prevalence of Depression and Anxiety in Iranian Patients With Diabetes Mellitus: A Systematic Review and Meta-Analysisselamat parminNo ratings yet
- Janssen COVID-19 Vaccine (Johnson & Johnson) : Vaccine Preparation and Administration SummaryDocument3 pagesJanssen COVID-19 Vaccine (Johnson & Johnson) : Vaccine Preparation and Administration SummaryJohn Alex SelorioNo ratings yet
- Couvade Syndrome and PseudocyesisDocument4 pagesCouvade Syndrome and PseudocyesisJustin Ahorro-DionisioNo ratings yet
- ToxicologyDocument15 pagesToxicologySarah JaneNo ratings yet
- Hypertensión Ese - Spin - Brochure - Rev. - 03 - LowDocument12 pagesHypertensión Ese - Spin - Brochure - Rev. - 03 - LowVICTOR losanNo ratings yet
- Wilcock 2008Document11 pagesWilcock 2008Nadia SaiNo ratings yet