You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Skin Anatomy and PhysiologyDocument5 pagesSkin Anatomy and PhysiologyKhan KamaalNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Chapter 45 Urinary EliminationDocument29 pagesChapter 45 Urinary EliminationKwenaNo ratings yet
- Pondicherry University Surgery Exam Syllabus and Expected QuestionsDocument17 pagesPondicherry University Surgery Exam Syllabus and Expected QuestionsDhanoush MşđNo ratings yet
- Endocrine SystemDocument35 pagesEndocrine SystemLinkNo ratings yet
- Grade 3 Science Quiz Bee ReviewerDocument1 pageGrade 3 Science Quiz Bee ReviewerJulie Magno Ismael88% (58)
- Case Study On Meninomyocele (Repaired) PDocument29 pagesCase Study On Meninomyocele (Repaired) Pcharanjit kaur100% (1)
- Tampakan Radiologi Dengan Efusi Pleura UnilateralDocument5 pagesTampakan Radiologi Dengan Efusi Pleura Unilateral1234qweasdfNo ratings yet
- Anatomy and Physiology of The Urinary Tract Relation To Host Defense and Microbal InfectionDocument29 pagesAnatomy and Physiology of The Urinary Tract Relation To Host Defense and Microbal InfectionNatiqa MutafaniaNo ratings yet
- Daftar Pustaka: ReportDocument1 pageDaftar Pustaka: Report1234qweasdfNo ratings yet
- Journal Reading Saraf - YoelDocument2 pagesJournal Reading Saraf - Yoel1234qweasdfNo ratings yet
- Psychiatry: Comprehensive Textbook ofDocument44 pagesPsychiatry: Comprehensive Textbook ofRiuin23No ratings yet
- Urinary Tract Infection in Postmenopausal WomenDocument8 pagesUrinary Tract Infection in Postmenopausal WomenNurulSyaidahNo ratings yet
- Stroke 2010 Morgenstern 2108 29Document47 pagesStroke 2010 Morgenstern 2108 29Pirabakar MahendranNo ratings yet
- Kevin Hardisto Hyialin Membran DiseaseDocument32 pagesKevin Hardisto Hyialin Membran Disease1234qweasdfNo ratings yet
- HF Focused Update On New Pharmacological Therapy - Final PDFDocument23 pagesHF Focused Update On New Pharmacological Therapy - Final PDF1234qweasdfNo ratings yet
- Carpal TunnelDocument1 pageCarpal TunnelKadek Rudita YasaNo ratings yet
- Journal Reading Saraf - YoelDocument2 pagesJournal Reading Saraf - Yoel1234qweasdfNo ratings yet
- 1749 FullDocument37 pages1749 Full1234qweasdfNo ratings yet
- KDIGO CKD-MBD Update - Public Review - Final PDFDocument62 pagesKDIGO CKD-MBD Update - Public Review - Final PDF1234qweasdfNo ratings yet
- 1749 FullDocument37 pages1749 Full1234qweasdfNo ratings yet
- AsdDocument31 pagesAsd1234qweasdfNo ratings yet
- International Headache Classification III ICHD III 2013 Beta 1Document180 pagesInternational Headache Classification III ICHD III 2013 Beta 1Fityan Aulia RahmanNo ratings yet
- E282 FullDocument36 pagesE282 Full1234qweasdfNo ratings yet
- filePV1009 Irizarry 2Document7 pagesfilePV1009 Irizarry 21234qweasdfNo ratings yet
- AcsDocument13 pagesAcs1234qweasdfNo ratings yet
- DeliriumDocument38 pagesDeliriumVicta RyzaNo ratings yet
- RespDocument2 pagesRespNicolaeDincaNo ratings yet
- Ultrastructure of The in Chronic: Lung HypoxiaDocument7 pagesUltrastructure of The in Chronic: Lung Hypoxia1234qweasdfNo ratings yet
- Mini-Cx: Liver and Kidney RuptureDocument14 pagesMini-Cx: Liver and Kidney RuptureMoch NizamNo ratings yet
- 3 The Integumentary System: Section IDocument18 pages3 The Integumentary System: Section IVõ ĐứcNo ratings yet
- TEXTO 2 ANO - jUNHO 09Document3 pagesTEXTO 2 ANO - jUNHO 09lucijonesNo ratings yet
- Test AMG Sem II EnglezaDocument3 pagesTest AMG Sem II EnglezaCCCAXANo ratings yet
- Latihan EkspertiseDocument40 pagesLatihan EkspertiseRoberto HutapeaNo ratings yet
- Lesson 7 Sci Ed 204 p2Document29 pagesLesson 7 Sci Ed 204 p2Allysa Marie SilbolNo ratings yet
- Cerebrum: By: Pedro E. Ampil, M.D.FPSA Department of Human Structural Biology Our Lady of Fatima UniversityDocument29 pagesCerebrum: By: Pedro E. Ampil, M.D.FPSA Department of Human Structural Biology Our Lady of Fatima UniversityPlaza Jeanine LouiseNo ratings yet
- Cardinal Manifestetions of Renal DiseaseDocument61 pagesCardinal Manifestetions of Renal Diseasekirubel deribNo ratings yet
- Functional Neuroanatomy and Clinical Neuroscience - Foundations For Understanding Disorders of Cognition and Behavior 2022Document465 pagesFunctional Neuroanatomy and Clinical Neuroscience - Foundations For Understanding Disorders of Cognition and Behavior 2022Eduardo RodriguezNo ratings yet
- Chapter 9Document15 pagesChapter 9NG SHER WYNN MoeNo ratings yet
- Histology Drawings PDFDocument19 pagesHistology Drawings PDFVishwanath Sinduvadi100% (1)
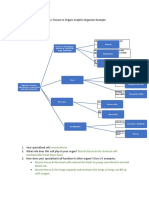
- Cells To Tissues To Organs Graphic Organizer ExampleDocument2 pagesCells To Tissues To Organs Graphic Organizer Exampleapi-431603797No ratings yet
- 3 MAJOR OPENINGS /right Atirum: Cardiovascular System Serious PericardiumDocument3 pages3 MAJOR OPENINGS /right Atirum: Cardiovascular System Serious PericardiumAebee Alcaraz100% (1)
- Nervous SystemDocument8 pagesNervous SystemNicah FranciscoNo ratings yet
- 8ad Science Yr 8Document16 pages8ad Science Yr 8maryamNo ratings yet
- Physiology Objectives DetailedDocument35 pagesPhysiology Objectives DetailedSOOOS94No ratings yet
- Transducer Frequency - 205/305/5.0 MHZ: DR Satish Kumar Sharma Consultant CardiologistDocument1 pageTransducer Frequency - 205/305/5.0 MHZ: DR Satish Kumar Sharma Consultant CardiologistHappyNo ratings yet
- Digestion and Absorption: Anatomy and Functions of the Human Digestive SystemDocument8 pagesDigestion and Absorption: Anatomy and Functions of the Human Digestive Systemzwindows123456789No ratings yet
- Review On Miracle of Herbals in Treatment and Regulation of ThyroidDocument5 pagesReview On Miracle of Herbals in Treatment and Regulation of ThyroidEditor IJTSRDNo ratings yet
- Adaption of Infants To Extra-Uterine LifeDocument10 pagesAdaption of Infants To Extra-Uterine LifeJulienne QuintaoNo ratings yet
- Alcoholic Liver DiseaseDocument9 pagesAlcoholic Liver DiseasePankaj DixitNo ratings yet
- Fisiologi Saraf OtonomDocument32 pagesFisiologi Saraf OtonomNiaNo ratings yet
- 1-Thyroid and Antithyroid Drugs (This)Document96 pages1-Thyroid and Antithyroid Drugs (This)hamidNo ratings yet
- HP4. Endocrine System - 100 - Ethan HelmDocument17 pagesHP4. Endocrine System - 100 - Ethan HelmNorPhea - នភាNo ratings yet