You might also like
- Professional Knowledge Questions For IBPS SO Marketing Mains 2017 10Document2 pagesProfessional Knowledge Questions For IBPS SO Marketing Mains 2017 10Arif MohammadNo ratings yet
- Finland Tops 2018 World Happiness Index; India Slips to 133rd RankDocument3 pagesFinland Tops 2018 World Happiness Index; India Slips to 133rd RankArif MohammadNo ratings yet
- Business Environment and Law PDFDocument452 pagesBusiness Environment and Law PDFrajeev sharmaNo ratings yet
- Professional Knowledge Questions For IBPS SO Marketing Mains 17Document2 pagesProfessional Knowledge Questions For IBPS SO Marketing Mains 17Arif MohammadNo ratings yet
- Professional Knowledge Questions For IBPS SO Marketing Mains 2017 6Document2 pagesProfessional Knowledge Questions For IBPS SO Marketing Mains 2017 6Arif MohammadNo ratings yet
- Professional Knowledge Questions For IBPS SO Marketing Mains 2017 7Document2 pagesProfessional Knowledge Questions For IBPS SO Marketing Mains 2017 7Arif MohammadNo ratings yet
- D 17 14 Paper 3 III (Management) Inst Cbse Net Dec 2014Document32 pagesD 17 14 Paper 3 III (Management) Inst Cbse Net Dec 2014DR.KUMAR PUNIT GOEL SIRNo ratings yet
- Professional Knowledge Questions For IBPS SO Marketing Mains 2017 4Document2 pagesProfessional Knowledge Questions For IBPS SO Marketing Mains 2017 4Arif MohammadNo ratings yet
- Professional Knowledge Questions For IBPS SO Marketing Mains 2017..Document2 pagesProfessional Knowledge Questions For IBPS SO Marketing Mains 2017..Arif MohammadNo ratings yet
- Professional Knowledge Questions For IBPS SO Marketing Mains 2017 13Document2 pagesProfessional Knowledge Questions For IBPS SO Marketing Mains 2017 13Arif MohammadNo ratings yet
- Professional Knowledge Questions For IBPS SO Marketing Mains 17Document2 pagesProfessional Knowledge Questions For IBPS SO Marketing Mains 17Arif MohammadNo ratings yet
- Professional Knowledge Questions For IBPS SO Marketing Mains 2017....Document2 pagesProfessional Knowledge Questions For IBPS SO Marketing Mains 2017....Arif MohammadNo ratings yet
- Professional Knowledge Questions For IBPS SO Marketing Mains 2017 12Document2 pagesProfessional Knowledge Questions For IBPS SO Marketing Mains 2017 12Arif MohammadNo ratings yet
- Professional Knowledge Questions For IBPS SO Marketing Mains 2017 2Document2 pagesProfessional Knowledge Questions For IBPS SO Marketing Mains 2017 2Arif MohammadNo ratings yet
- Professional Knowledge Questions For IBPS SO Marketing Mains 2017Document2 pagesProfessional Knowledge Questions For IBPS SO Marketing Mains 2017Arif MohammadNo ratings yet
- Professional Knowledge Questions For IBPS SO MKTG Mains 2017Document2 pagesProfessional Knowledge Questions For IBPS SO MKTG Mains 2017Arif MohammadNo ratings yet
- Chapter 9Document42 pagesChapter 9prasenajita2618No ratings yet
- Multifocal Pha Kic ImplantDocument6 pagesMultifocal Pha Kic ImplantArif MohammadNo ratings yet
- Awards Honours 2017Document31 pagesAwards Honours 2017Arif MohammadNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Monday Supplement 8 Pages - San Diego 2011 For WebDocument8 pagesMonday Supplement 8 Pages - San Diego 2011 For WebArif MohammadNo ratings yet
- Uday India - August 13 2017 PDFDocument52 pagesUday India - August 13 2017 PDFArif MohammadNo ratings yet
- Basic concepts of computers explainedDocument32 pagesBasic concepts of computers explainedabhi_txt90No ratings yet
- Bank Exam Portal: M.Tech/B.Tech AdmissionDocument10 pagesBank Exam Portal: M.Tech/B.Tech AdmissionArif MohammadNo ratings yet
- SSC CGL Tier-2 AAO Exam Syllabus Finance EconomicsDocument3 pagesSSC CGL Tier-2 AAO Exam Syllabus Finance EconomicsArif MohammadNo ratings yet
- Uday India August 13 2017Document52 pagesUday India August 13 2017Arif MohammadNo ratings yet
- Journal Casereport 1Document5 pagesJournal Casereport 1Arif MohammadNo ratings yet
- PhakikiolDocument1 pagePhakikiolArif MohammadNo ratings yet
- BSC September 2017Document131 pagesBSC September 2017Arif MohammadNo ratings yet
- Overview of Phakic Iols: Cover StoryDocument5 pagesOverview of Phakic Iols: Cover StoryArif MohammadNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- High-Resolution Transmission Electron Microscopy (Hrtem) Study of The 4A and 6A Superstructure of Bornite Cu FesDocument9 pagesHigh-Resolution Transmission Electron Microscopy (Hrtem) Study of The 4A and 6A Superstructure of Bornite Cu FesJarar HaiderNo ratings yet
- Ultrasonic Testing Ut Q Bank A-4Document10 pagesUltrasonic Testing Ut Q Bank A-4kingstonNo ratings yet
- BIOCHEMISTRY ANALYZERS GUIDEDocument38 pagesBIOCHEMISTRY ANALYZERS GUIDEAdam WARESHALLEENo ratings yet
- AESTHETICS LASER PORTFOLIO - Quanta System - PDF Catalogs - Technical DocumentationDocument7 pagesAESTHETICS LASER PORTFOLIO - Quanta System - PDF Catalogs - Technical DocumentationMunir AldeekNo ratings yet
- Gaussian Beam OpticsDocument12 pagesGaussian Beam OpticsHanh MaiNo ratings yet
- MITRAS Transmissometer Operator Training GuideDocument90 pagesMITRAS Transmissometer Operator Training GuideM. Abdullah Reza D.HNo ratings yet
- Tutorial 1Document2 pagesTutorial 1Rajesh AjayNo ratings yet
- Low Cost AFM Piezo BusserDocument11 pagesLow Cost AFM Piezo Busserjast_80No ratings yet
- SPL S4l90a - 3 A01 - enDocument20 pagesSPL S4l90a - 3 A01 - enAndrey LapshovNo ratings yet
- BG Birds PreviewDocument21 pagesBG Birds PreviewAlfredo GonzalezNo ratings yet
- Glossary of Terms For Fiber Optics CableDocument5 pagesGlossary of Terms For Fiber Optics CableAli UsmanNo ratings yet
- What Digital Camera - September 2016Document100 pagesWhat Digital Camera - September 2016Voinea AndreiNo ratings yet
- 1568005103545-TCT - 4 - OFC PrinciplesDocument156 pages1568005103545-TCT - 4 - OFC Principlesvinay0ranaNo ratings yet
- Color Picker - CoolorsDocument1 pageColor Picker - CoolorsHannah ShanelleNo ratings yet
- Micr Biology: Observing Microorganisms Through A MicroscopeDocument31 pagesMicr Biology: Observing Microorganisms Through A MicroscopeMich ElleNo ratings yet
- Moptim IRef Brochure enDocument3 pagesMoptim IRef Brochure enDiego A. Pérez CruzNo ratings yet
- DS-2CE16H0T-ITPFS 5 MP Audio CameraDocument4 pagesDS-2CE16H0T-ITPFS 5 MP Audio CameraChristian Rios GuevaraNo ratings yet
- Parallel Beam Convergent Beam Divergent BeamDocument16 pagesParallel Beam Convergent Beam Divergent BeamNaman YadavNo ratings yet
- Reiser 1988Document5 pagesReiser 1988peng wangNo ratings yet
- Yang 2012 NatcomDocument7 pagesYang 2012 NatcomAthan CalugayNo ratings yet
- Photogrammetric Applications For Cultural HeritageDocument128 pagesPhotogrammetric Applications For Cultural HeritageKathy JancesNo ratings yet
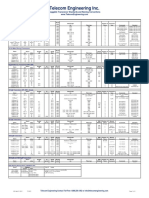
- Telecom Engineering Inc.: Pluggable Transciever Standards and Naming ConventionsDocument2 pagesTelecom Engineering Inc.: Pluggable Transciever Standards and Naming ConventionsRonald AcostaNo ratings yet
- Jam PH2021Document20 pagesJam PH2021Rahul Satapathy100% (1)
- DLP Science 7 3rd Quarter LightDocument2 pagesDLP Science 7 3rd Quarter LightDongBacabis90% (10)
- AcoustoOptics, Adrian KorpelDocument349 pagesAcoustoOptics, Adrian KorpelDiana Félix100% (2)
- 빛공해 방지를 위한 조명기구 설치·관리 권고기준 가이드라인Document114 pages빛공해 방지를 위한 조명기구 설치·관리 권고기준 가이드라인ByungHoon JungNo ratings yet
- FRET (Fluorescence Resonance Energy Transfer) Q&ADocument3 pagesFRET (Fluorescence Resonance Energy Transfer) Q&AVeena mitraNo ratings yet
- Fast-Fourier-transform Based Numerical Integration Method For The Rayleigh-Sommerfeld Diffraction FormulaDocument9 pagesFast-Fourier-transform Based Numerical Integration Method For The Rayleigh-Sommerfeld Diffraction Formulaluo wangNo ratings yet
- 3.3.1.1 Progressive WavesDocument62 pages3.3.1.1 Progressive WavesotwadiNo ratings yet
- Laser Telemetric SystemDocument5 pagesLaser Telemetric SystemDurai Raj100% (1)