You might also like
- PSB 368Document6 pagesPSB 368Miguel Cuevas DolotNo ratings yet
- Effectiveness of Transdermal MagnesiumDocument2 pagesEffectiveness of Transdermal MagnesiumMiguel Cuevas Dolot100% (1)
- (MED) COVID-19 Trans V. 2.0Document6 pages(MED) COVID-19 Trans V. 2.0Isabel VinasNo ratings yet
- How Can Patients Visitors Help - May18Document2 pagesHow Can Patients Visitors Help - May18Miguel Cuevas DolotNo ratings yet
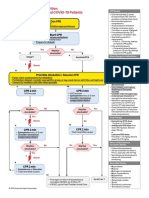
- ACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsDocument1 pageACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsMariuxi Tatiana ChocoNo ratings yet
- Covid 19 CPR 7 RulesDocument21 pagesCovid 19 CPR 7 RulesMiguel Cuevas DolotNo ratings yet
- Covid 19 CPR 7 RulesDocument21 pagesCovid 19 CPR 7 RulesMiguel Cuevas DolotNo ratings yet
- Clinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Document30 pagesClinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Ekambaram TrmNo ratings yet
- Physical Examination in ENT: Ussana Promyothin, MDDocument60 pagesPhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotNo ratings yet
- Covid 19 PDFDocument18 pagesCovid 19 PDFMiguel Cuevas DolotNo ratings yet
- Physical Examination in ENT: Ussana Promyothin, MDDocument60 pagesPhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotNo ratings yet
- Physical Assessment: Ear, Nose, Mouth, and ThroatDocument59 pagesPhysical Assessment: Ear, Nose, Mouth, and ThroatMiguel Cuevas DolotNo ratings yet
- Vertigo Gail Ishiyama 1 13 10Document40 pagesVertigo Gail Ishiyama 1 13 10Myname Rama LienNo ratings yet
- Cook Book (Filipino) 13 PDFDocument23 pagesCook Book (Filipino) 13 PDFAdina AnghelNo ratings yet
- Clinical AbstractDocument4 pagesClinical AbstractMiguel Cuevas DolotNo ratings yet
- Pedia Tickler Update 2017Document2 pagesPedia Tickler Update 2017Tani BokNo ratings yet
- Active Listening HANDOUT PDFDocument26 pagesActive Listening HANDOUT PDFMiguel Cuevas DolotNo ratings yet
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFDocument12 pagesA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotNo ratings yet
- HEMAreviewDocument3 pagesHEMAreviewMiguel Cuevas DolotNo ratings yet
- Benign Paroxysmal Positional Vertigo: Waseem WatadDocument37 pagesBenign Paroxysmal Positional Vertigo: Waseem WatadnoviNo ratings yet
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFDocument12 pagesA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotNo ratings yet
- Drug IndexDocument2 pagesDrug IndexMiguel Cuevas DolotNo ratings yet
- Nocturnals Physiology 2018Document14 pagesNocturnals Physiology 2018Miguel Cuevas DolotNo ratings yet
- Neurologic ExamDocument1 pageNeurologic ExamMiguel Cuevas DolotNo ratings yet
- History Taking ExaminationDocument7 pagesHistory Taking ExaminationIndunil AnuruddhikaNo ratings yet
- Community-Acquired Pneumonia - CPG 2016Document26 pagesCommunity-Acquired Pneumonia - CPG 2016Jamie SebastianNo ratings yet
- TCVS - Cardiac Surgery Part 2 Dr. de AsisDocument8 pagesTCVS - Cardiac Surgery Part 2 Dr. de AsisMiguel Cuevas DolotNo ratings yet
- Anesthesia Pocket Cards 7 18 18Document6 pagesAnesthesia Pocket Cards 7 18 18Miguel Cuevas DolotNo ratings yet
- Kerosene PDFDocument31 pagesKerosene PDFRudyMLanaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Cristy Santos BOMDocument111 pagesCristy Santos BOMLito ObstaculoNo ratings yet
- Pediatrics Care Plan Kawasaki Disease Final Draft and CorrectedDocument9 pagesPediatrics Care Plan Kawasaki Disease Final Draft and CorrectedValencia Vickers50% (4)
- Austere Medicine Books PDFDocument10 pagesAustere Medicine Books PDFmorrischuck100% (1)
- The Black PlagueDocument3 pagesThe Black PlagueKevin MoralesNo ratings yet
- COVID-19: Simple Answers To Top Questions: Risk Communication Field Guide Questions and Key MessagesDocument128 pagesCOVID-19: Simple Answers To Top Questions: Risk Communication Field Guide Questions and Key MessagesJazzyNo ratings yet
- Cause & Effect - Louise Joseph G. PeraltaDocument4 pagesCause & Effect - Louise Joseph G. PeraltaLouise Joseph G. PeraltaNo ratings yet
- InTech-Molar Incisor Hypomineralization Morphological Aetiological Epidemiological and Clinical ConsiderationsDocument25 pagesInTech-Molar Incisor Hypomineralization Morphological Aetiological Epidemiological and Clinical ConsiderationsNeagu EmaNo ratings yet
- Chapter 2Document14 pagesChapter 2JM ElleNo ratings yet
- Child Attitude Joward Jllness Scale: EspaňDocument1 pageChild Attitude Joward Jllness Scale: EspaňAvinash ToraneNo ratings yet
- Dengue Lecture For SibalomDocument48 pagesDengue Lecture For SibalomCzerwin JualesNo ratings yet
- Domestic Rabbits Diseases and ParasitesDocument31 pagesDomestic Rabbits Diseases and ParasitesAlvaro Pauchard Pino100% (1)
- Diagnostic Terms For Pulp Conditions - JoE 2009Document13 pagesDiagnostic Terms For Pulp Conditions - JoE 2009Bicho Angel LisseaNo ratings yet
- Jurnal Case Report - Hemangioma KavernosaDocument12 pagesJurnal Case Report - Hemangioma KavernosaMaulida Ayu NorizaNo ratings yet
- Cocci VexDocument18 pagesCocci VexNona AlyNo ratings yet
- BMC Public Health: Which Preventive Measures Might Protect Health Care Workers From SARS?Document8 pagesBMC Public Health: Which Preventive Measures Might Protect Health Care Workers From SARS?Rahel YaserNo ratings yet
- Handbook of Disease Burdens and Quality of Life Measures - V. Preedy, R. Watson (Springer, 2010) WWDocument4,278 pagesHandbook of Disease Burdens and Quality of Life Measures - V. Preedy, R. Watson (Springer, 2010) WWRiska Indriani100% (1)
- Carcinogenesis: Robbins Basic Pathology, 7 Kumar, Cotran, RobbinsDocument29 pagesCarcinogenesis: Robbins Basic Pathology, 7 Kumar, Cotran, RobbinsHairon DhiyaulhaqNo ratings yet
- Navel DisplacementDocument4 pagesNavel Displacementdinesh100% (1)
- Parasites, How To Eliminate Them NaturallyDocument44 pagesParasites, How To Eliminate Them NaturallyXuxuxel100% (3)
- Catastrophic Health Expenditure of Middle Class in India Due To Covid-19Document3 pagesCatastrophic Health Expenditure of Middle Class in India Due To Covid-19Ashwini PoojaryNo ratings yet
- CKD (F&e)Document110 pagesCKD (F&e)Al-nazer Azer Al100% (1)
- Glomerular DiseaseDocument24 pagesGlomerular DiseasemadhuNo ratings yet
- Keilitis Eksfoliatif JurnalDocument7 pagesKeilitis Eksfoliatif JurnalLeni Aria NastaNo ratings yet
- ManiaaDocument3 pagesManiaaadityanarang147No ratings yet
- Jen Ipcr 1st QuarterDocument4 pagesJen Ipcr 1st QuarterJairolla ObayNo ratings yet
- Entry Form: Hospital Best Practices in Infection Prevention and Control Awards Year ViDocument1 pageEntry Form: Hospital Best Practices in Infection Prevention and Control Awards Year ViPeepsNo ratings yet
- WHY NOT BHARAT RATNA TO GREAT MEDICAL SCIENTIST AND MAN OF MIRACLE DRUGS DR - YELLAPRAGADA SUBBA RAO ?Document13 pagesWHY NOT BHARAT RATNA TO GREAT MEDICAL SCIENTIST AND MAN OF MIRACLE DRUGS DR - YELLAPRAGADA SUBBA RAO ?Anumakonda JagadeeshNo ratings yet
- Dyspepsia (Gastritis) Case StudiesDocument9 pagesDyspepsia (Gastritis) Case StudiesJessica Nurin Graman100% (1)
- School Entry Health Exam Form FL (Sample)Document2 pagesSchool Entry Health Exam Form FL (Sample)chase1828No ratings yet
- Comparison of Goldmann Applanation Tonometer, Tono-PenDocument19 pagesComparison of Goldmann Applanation Tonometer, Tono-PenLidiasilambaNo ratings yet