You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- New Newstart 2Document1 pageNew Newstart 2Adrian KhomanNo ratings yet
- Practical Algorithms in Pediatric Hematology and OncologyDocument119 pagesPractical Algorithms in Pediatric Hematology and OncologyNubia Ahumadaa100% (5)
- IM Shelf - AmbossDocument61 pagesIM Shelf - AmbossHaadi AliNo ratings yet
- Alarp Risk Assessment SampleDocument7 pagesAlarp Risk Assessment SampleCriticalEyeNo ratings yet
- Fetal Heart Defects and Measures of Cerebral Size: Objectives Study DesignDocument8 pagesFetal Heart Defects and Measures of Cerebral Size: Objectives Study DesignAdrian KhomanNo ratings yet
- 10 1002@ppul 1950160309 PDFDocument13 pages10 1002@ppul 1950160309 PDFAdrian KhomanNo ratings yet
- Merrill 2004Document9 pagesMerrill 2004Adrian KhomanNo ratings yet
- Be Rent Sen 2015Document12 pagesBe Rent Sen 2015Adrian KhomanNo ratings yet
- Jurnal Neuroo Wanigasinghe2015Document7 pagesJurnal Neuroo Wanigasinghe2015melly adityaNo ratings yet
- Danne 2018Document54 pagesDanne 2018Adrian KhomanNo ratings yet
- DHF Menurut WHO 2011Document212 pagesDHF Menurut WHO 2011Jamal SutrisnaNo ratings yet
- Chronic Lung Disease in Premature BabiesDocument2 pagesChronic Lung Disease in Premature BabiesAdrian KhomanNo ratings yet
- Chronic Lung Disease in Premature BabiesDocument2 pagesChronic Lung Disease in Premature BabiesAdrian KhomanNo ratings yet
- Kugelman2007 PDFDocument7 pagesKugelman2007 PDFAdrian KhomanNo ratings yet
- BLT 15 259Document9 pagesBLT 15 259Adrian KhomanNo ratings yet
- Be Rent Sen 2015Document12 pagesBe Rent Sen 2015Adrian KhomanNo ratings yet
- Pocket Pediatrics Handbook for Children by MGHDocument5 pagesPocket Pediatrics Handbook for Children by MGHAdrian KhomanNo ratings yet
- Alan Sari 2016Document11 pagesAlan Sari 2016Adrian KhomanNo ratings yet
- Status Nutrisi WHO Laki-LakiDocument1 pageStatus Nutrisi WHO Laki-LakiAdrian KhomanNo ratings yet
- Jae 201174012905Document5 pagesJae 201174012905Adrian KhomanNo ratings yet
- Miaoying Zhang, Xiaojing Li, Li Xi, Zhuhui Zhao, Ruoqian Cheng, Bingbing Wu and Feihong LuoDocument1 pageMiaoying Zhang, Xiaojing Li, Li Xi, Zhuhui Zhao, Ruoqian Cheng, Bingbing Wu and Feihong LuoAdrian KhomanNo ratings yet
- Treatment of Autoimmune Hemolytic Anemias, 2014 ReviewDocument8 pagesTreatment of Autoimmune Hemolytic Anemias, 2014 ReviewSabina UlubeanuNo ratings yet
- Ehz 467Document65 pagesEhz 467Coy Calapatia-TorresNo ratings yet
- Pediatric Cardiology: Original ArticlesDocument5 pagesPediatric Cardiology: Original ArticlesAdrian KhomanNo ratings yet
- United States Patent (19) 11 Patent Number: 5,969,606: Reber Et Al. (45) Date of Patent: Oct. 19, 1999Document12 pagesUnited States Patent (19) 11 Patent Number: 5,969,606: Reber Et Al. (45) Date of Patent: Oct. 19, 1999Adrian KhomanNo ratings yet
- Treatment of Autoimmune Hemolytic Anemias, 2014 ReviewDocument8 pagesTreatment of Autoimmune Hemolytic Anemias, 2014 ReviewSabina UlubeanuNo ratings yet
- Hemodynamic Study: O Content (mL/100 ML) HB × 1.36 × (O Sat/100)Document9 pagesHemodynamic Study: O Content (mL/100 ML) HB × 1.36 × (O Sat/100)Adrian KhomanNo ratings yet
- Pediatric Neurology: Hye-Ryun Yeh MD, Min-Jee Kim MD, Tae-Sung Ko MD, PHD, Mi-Sun Yum MD, PHD, Su-Jeong You MD, PHDDocument6 pagesPediatric Neurology: Hye-Ryun Yeh MD, Min-Jee Kim MD, Tae-Sung Ko MD, PHD, Mi-Sun Yum MD, PHD, Su-Jeong You MD, PHDAdrian KhomanNo ratings yet
- Diagnostic and Therapeutic Challenges of Primary Autoimmune Haemolytic Anaemia in ChildrenDocument7 pagesDiagnostic and Therapeutic Challenges of Primary Autoimmune Haemolytic Anaemia in ChildrenAdrian KhomanNo ratings yet
- United States Patent (19) 11 Patent Number: 5,969,606: Reber Et Al. (45) Date of Patent: Oct. 19, 1999Document12 pagesUnited States Patent (19) 11 Patent Number: 5,969,606: Reber Et Al. (45) Date of Patent: Oct. 19, 1999Adrian KhomanNo ratings yet
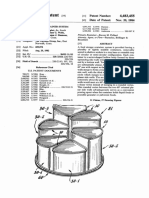
- Food storage container system patentDocument13 pagesFood storage container system patentAdrian KhomanNo ratings yet
- Breastfeeding Rates and Programs in Europe: A Survey of 11 National Breastfeeding Committees and RepresentativesDocument8 pagesBreastfeeding Rates and Programs in Europe: A Survey of 11 National Breastfeeding Committees and RepresentativesAdrian KhomanNo ratings yet
- Cebu Normal University College of NursingDocument7 pagesCebu Normal University College of NursingGwyn RosalesNo ratings yet
- What Is Down SyndromeDocument4 pagesWhat Is Down SyndromeJanica GonzalesNo ratings yet
- Nurture and ConnectionDocument4 pagesNurture and Connectionparents021100% (1)
- Aur VedaDocument4 pagesAur VedaLalit MishraNo ratings yet
- Subcutaneous MycosesDocument23 pagesSubcutaneous Mycosessarguss14100% (1)
- Pharmacoeconomics - Part IIIDocument29 pagesPharmacoeconomics - Part IIISima JabbariNo ratings yet
- 45 PDFDocument8 pages45 PDFChika FebrianiNo ratings yet
- Fall Risk Care Plan NHS PDFDocument2 pagesFall Risk Care Plan NHS PDFBelayetNo ratings yet
- Tibbonto: Knowledge Representation of Prophet Medicine (Tibb Al-Nabawi)Document5 pagesTibbonto: Knowledge Representation of Prophet Medicine (Tibb Al-Nabawi)INFOPARK CSCNo ratings yet
- Severe Gastric ImpactionDocument4 pagesSevere Gastric ImpactionNanda Ayu Cindy KashiwabaraNo ratings yet
- R - MN R - 1 Z: Mkg-Xixltechlib/1 T/06Document48 pagesR - MN R - 1 Z: Mkg-Xixltechlib/1 T/06Jhantu MazumderNo ratings yet
- Development of Push-Pull Osmotic Pump Tablets For A SlightlyDocument4 pagesDevelopment of Push-Pull Osmotic Pump Tablets For A SlightlyphamuyenthuNo ratings yet
- Annexure 'CD - 01' FORMAT FOR COURSE CURRICULUMDocument4 pagesAnnexure 'CD - 01' FORMAT FOR COURSE CURRICULUMYash TiwariNo ratings yet
- Montelukast SodiumDocument10 pagesMontelukast SodiumikhasilNo ratings yet
- The Abc of Handover: E.D. Registrar A: Areas AllocationDocument1 pageThe Abc of Handover: E.D. Registrar A: Areas AllocationDiahNiatiNo ratings yet
- Mnemonics For PharmacologyDocument46 pagesMnemonics For PharmacologysnehaNo ratings yet
- Phobiasgalore1 2Document2 pagesPhobiasgalore1 2api-264827695No ratings yet
- Endoscopic Ethmoidectomy - FESS - Surgical TechniqueDocument30 pagesEndoscopic Ethmoidectomy - FESS - Surgical TechniqueSaurav GurungNo ratings yet
- Intro Tothe Function of Parathyroid Gland, ConciseDocument34 pagesIntro Tothe Function of Parathyroid Gland, Conciseinka.elseNo ratings yet
- R3 Vital Pulp Therapy With New MaterialsDocument7 pagesR3 Vital Pulp Therapy With New MaterialsWening TyasNo ratings yet
- Radiographic EvaluationDocument12 pagesRadiographic EvaluationLuis Gerardo Castillo MendozaNo ratings yet
- Fphar 12 768268Document25 pagesFphar 12 768268Araceli Anaya AlvaradoNo ratings yet
- Annexure-II-2013 2 1Document1,218 pagesAnnexure-II-2013 2 1bala11ap4598No ratings yet
- Morning Report (Cardiology) : On Duty: Nadya Julaifa, Nadya Julaifa Supervisor: Dr. Yusra Pintaningrum, Sp. JP (K) FIHADocument16 pagesMorning Report (Cardiology) : On Duty: Nadya Julaifa, Nadya Julaifa Supervisor: Dr. Yusra Pintaningrum, Sp. JP (K) FIHAAdisti NurutamiNo ratings yet
- Multiple Births Definition, Causes & CareDocument11 pagesMultiple Births Definition, Causes & CareCacing UcilNo ratings yet
- Guide Sondes Logiq s8Document4 pagesGuide Sondes Logiq s8mahfoudNo ratings yet
- Stroke Awareness EducationDocument7 pagesStroke Awareness EducationIneke PutriNo ratings yet
- Drug StudyDocument17 pagesDrug StudyJoan RabeNo ratings yet