You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Microbial Interactions With The Host in Periodontal DiseasesDocument74 pagesMicrobial Interactions With The Host in Periodontal Diseasesrupali100% (2)
- Kepustakaan Lapsus Perforasi GasterDocument1 pageKepustakaan Lapsus Perforasi GasterSebiye OdaqNo ratings yet
- Long-term immune effects of tonsillectomy in childrenDocument1 pageLong-term immune effects of tonsillectomy in childrenSebiye OdaqNo ratings yet
- Follow Up Pasien Perforasi GasterDocument12 pagesFollow Up Pasien Perforasi GasterSebiye OdaqNo ratings yet
- Miso Vs Kuret PDFDocument4 pagesMiso Vs Kuret PDFSebiye OdaqNo ratings yet
- Int J Pediatr OtorhinolaryngolDocument1 pageInt J Pediatr OtorhinolaryngolSebiye OdaqNo ratings yet
- Follow Up Pasien Perforasi GasterDocument12 pagesFollow Up Pasien Perforasi GasterSebiye OdaqNo ratings yet
- DPDocument1 pageDPSebiye OdaqNo ratings yet
- Latar BelakangDocument11 pagesLatar BelakangSebiye OdaqNo ratings yet
- Latar BelakangDocument11 pagesLatar BelakangSebiye OdaqNo ratings yet
- Hosts UmbrellaDocument1 pageHosts UmbrellaFabsor SoralNo ratings yet
- Kepustakaan Lapsus Perforasi GasterDocument1 pageKepustakaan Lapsus Perforasi GasterSebiye OdaqNo ratings yet
- Omphalocele and GastroschisisDocument12 pagesOmphalocele and Gastroschisisluisisea100% (1)
- Long-Term Impacts of Tonsillectomy on Immune FunctionsDocument1 pageLong-Term Impacts of Tonsillectomy on Immune FunctionsSebiye OdaqNo ratings yet
- Kumpulan Emoticon Symbols DanDocument2 pagesKumpulan Emoticon Symbols DanSebiye OdaqNo ratings yet
- Percentile BB - U Dan TB - U PDFDocument1 pagePercentile BB - U Dan TB - U PDFQonita NahdiyahNo ratings yet
- Omphalocele and GastroschisisDocument12 pagesOmphalocele and Gastroschisisluisisea100% (1)
- Postgrad Med J 2005 Dec 81 (962) 772-6, Figure 1Document1 pagePostgrad Med J 2005 Dec 81 (962) 772-6, Figure 1Sebiye OdaqNo ratings yet
- Omphalocele and GastroschisisDocument12 pagesOmphalocele and Gastroschisisluisisea100% (1)
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Postgrad Med J 2005 Dec 81 (962) 772-6, Figure 1Document1 pagePostgrad Med J 2005 Dec 81 (962) 772-6, Figure 1Sebiye OdaqNo ratings yet
- Pruritus in Keloid Scars Mechanisms and Treatments-1Document20 pagesPruritus in Keloid Scars Mechanisms and Treatments-1widapnNo ratings yet
- Diabetic Kidney DiseaseDocument22 pagesDiabetic Kidney Diseasenadyamulya100% (1)
- TB4-Frag A Collection of StudiesDocument20 pagesTB4-Frag A Collection of StudiesscribdNo ratings yet
- Art. DanazolDocument9 pagesArt. DanazolmrintraNo ratings yet
- 6 Hos CarcinogenesisDocument90 pages6 Hos CarcinogenesisalgutNo ratings yet
- Pharmacology & TherapeuticsDocument12 pagesPharmacology & TherapeuticsWahyu Ika WardhaniNo ratings yet
- Advances in Medical SciencesDocument4 pagesAdvances in Medical SciencesMuhammad AdithiaNo ratings yet
- Physical Therapy and Precision Rehabilitation in Shoulder Rotator Cuff DiseaseDocument11 pagesPhysical Therapy and Precision Rehabilitation in Shoulder Rotator Cuff DiseaseAlvaro AlarconNo ratings yet
- Aging of The Male Reproductive System: M. Hermann, G. Untergasser, H. Rumpold, P. BergerDocument13 pagesAging of The Male Reproductive System: M. Hermann, G. Untergasser, H. Rumpold, P. BergerAnonymous pzkcmBNo ratings yet
- Cirrosis LANCET 2008Document14 pagesCirrosis LANCET 2008Natalia ElizabethNo ratings yet
- Proinflammatory Cytokines and Periodontal DiseaseDocument6 pagesProinflammatory Cytokines and Periodontal DiseasePeertechz Publications Inc.No ratings yet
- Studiu EumastosDocument8 pagesStudiu EumastosIoana VztNo ratings yet
- Download ebook Allergy Essentials 2Nd Edition Pdf full chapter pdfDocument67 pagesDownload ebook Allergy Essentials 2Nd Edition Pdf full chapter pdfjames.odell240100% (24)
- David Gate CV 9-19-18Document5 pagesDavid Gate CV 9-19-18David GateNo ratings yet
- Advanced Glycation End Products (AGEs) and Other Adducts in Aging-Related Diseases and Alcohol-Mediated Tissue InjuryDocument21 pagesAdvanced Glycation End Products (AGEs) and Other Adducts in Aging-Related Diseases and Alcohol-Mediated Tissue Injurysorin.morosan64No ratings yet
- CarcinogenDocument196 pagesCarcinogenJosé RamírezNo ratings yet
- Pathology of The Bile Duct 2017 - Yasuni Nakanuma PDFDocument215 pagesPathology of The Bile Duct 2017 - Yasuni Nakanuma PDFHîrjoabă IoanNo ratings yet
- Addis Ababa University School of Graduate Studies: October, 2011Document58 pagesAddis Ababa University School of Graduate Studies: October, 2011KenesaNo ratings yet
- Ntestinal Intraepithelial LymphocytesDocument21 pagesNtestinal Intraepithelial LymphocytesEDGAR FUENMAYOR PIRELANo ratings yet
- Artigo OncoDocument14 pagesArtigo OncoCatarina LuísNo ratings yet
- Radiation-Induced Lung Injury - UpToDateDocument38 pagesRadiation-Induced Lung Injury - UpToDateTatiana Valencia CastañoNo ratings yet
- Mechanisms of Glomerular Crescent FormationDocument19 pagesMechanisms of Glomerular Crescent Formation_siegfried_No ratings yet
- Neuroinflammation in Alzheimer's DiseaseDocument36 pagesNeuroinflammation in Alzheimer's DiseaseRamon LopesNo ratings yet
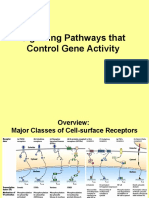
- 16) Signaling Pathways That Control Gene ActivityDocument27 pages16) Signaling Pathways That Control Gene ActivityRNo ratings yet
- WOUND HEALING AND REPAIR PROCESSDocument67 pagesWOUND HEALING AND REPAIR PROCESSAnicet MwaitalaNo ratings yet
- A Follicular Regulatory Innate Lymphoid Cell Population Impairs Interactions Between Germinal Center TFH and B CellsDocument13 pagesA Follicular Regulatory Innate Lymphoid Cell Population Impairs Interactions Between Germinal Center TFH and B Cellsiva hullNo ratings yet
- Levin - Godukhin - 2017 - Modulating Effect of Cytokines On Mechanisms of Synaptic Plasticity in The BrainDocument11 pagesLevin - Godukhin - 2017 - Modulating Effect of Cytokines On Mechanisms of Synaptic Plasticity in The Brainkeon.arbabi.altNo ratings yet
- Kim 2016Document7 pagesKim 2016yolanda tejaNo ratings yet
- Perineural Invasion Molecular MechanismsDocument21 pagesPerineural Invasion Molecular MechanismsgangligonNo ratings yet