You might also like
- Carcinogens - Carcinogens by Sites of Body (IARC) PDFDocument1 pageCarcinogens - Carcinogens by Sites of Body (IARC) PDFItharshan IndreswaranNo ratings yet
- Gastroeneteritis - Pediatrics (Nelson's)Document20 pagesGastroeneteritis - Pediatrics (Nelson's)Itharshan IndreswaranNo ratings yet
- Pharmacology - Anti-Inflammatory Drugs - Corticosteroid, NSAID, Leukotriene (Eicosanoids)Document9 pagesPharmacology - Anti-Inflammatory Drugs - Corticosteroid, NSAID, Leukotriene (Eicosanoids)Itharshan IndreswaranNo ratings yet
- Rash - Severely Ill (Differentials) PDFDocument11 pagesRash - Severely Ill (Differentials) PDFItharshan IndreswaranNo ratings yet
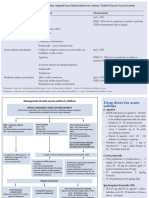
- Acute Severe Asthma Hospital ManagementDocument1 pageAcute Severe Asthma Hospital ManagementItharshan IndreswaranNo ratings yet
- Herbal Approach to Managing Polycystic Ovarian Syndrome (PCOS) SymptomsDocument1 pageHerbal Approach to Managing Polycystic Ovarian Syndrome (PCOS) SymptomsItharshan IndreswaranNo ratings yet
- Asthma (Acute) Management - Children (Pediatrics)Document2 pagesAsthma (Acute) Management - Children (Pediatrics)Itharshan IndreswaranNo ratings yet
- Amenorrhea - Algorithm & DifferentialsDocument9 pagesAmenorrhea - Algorithm & DifferentialsItharshan IndreswaranNo ratings yet
- Bradycardia PDFDocument1 pageBradycardia PDFItharshan IndreswaranNo ratings yet
- Spirometry Curve Errors Correction PDFDocument1 pageSpirometry Curve Errors Correction PDFItharshan IndreswaranNo ratings yet
- Circulatory System - Arterial & Venous TreesDocument28 pagesCirculatory System - Arterial & Venous TreesItharshan IndreswaranNo ratings yet
- Cardiovascular Regulation - PhysiologyDocument9 pagesCardiovascular Regulation - PhysiologyItharshan IndreswaranNo ratings yet
- Martyrs Park PDFDocument5 pagesMartyrs Park PDFItharshan IndreswaranNo ratings yet
- Abdomen Diagnoses PDFDocument2 pagesAbdomen Diagnoses PDFLaura Lopez RocaNo ratings yet
- Acute Severe Asthma Hospital ManagementDocument1 pageAcute Severe Asthma Hospital ManagementItharshan IndreswaranNo ratings yet
- Introduction in Human ParasitologyDocument53 pagesIntroduction in Human ParasitologyItharshan IndreswaranNo ratings yet
- Poster2 Arrhythmia Recognition eDocument1 pagePoster2 Arrhythmia Recognition eItharshan IndreswaranNo ratings yet
- Pharmacology - Mnemonics PDFDocument140 pagesPharmacology - Mnemonics PDFItharshan Indreswaran76% (17)
- Normal Lab Values GuideDocument2 pagesNormal Lab Values GuideItharshan Indreswaran83% (18)
- Martyrs ParkDocument6 pagesMartyrs ParkItharshan IndreswaranNo ratings yet
- Martyrs Park PDFDocument5 pagesMartyrs Park PDFItharshan IndreswaranNo ratings yet
- Pharmacology - Mnemonics PDFDocument140 pagesPharmacology - Mnemonics PDFItharshan Indreswaran76% (17)
- Introduction To Chinese Society and CultureDocument5 pagesIntroduction To Chinese Society and CultureItharshan IndreswaranNo ratings yet
- Abdominal Aorta SonogramDocument3 pagesAbdominal Aorta SonogramItharshan IndreswaranNo ratings yet
- Chapter 22Document14 pagesChapter 22Itharshan IndreswaranNo ratings yet
- Pulm 2005 Exam QuestionsDocument32 pagesPulm 2005 Exam QuestionsItharshan IndreswaranNo ratings yet
- Classification of Cardiac MurmursDocument1 pageClassification of Cardiac MurmursItharshan IndreswaranNo ratings yet
- General PathologyDocument261 pagesGeneral PathologyHanif SharNo ratings yet
- Pharmacology: For Health Science StudentsDocument211 pagesPharmacology: For Health Science StudentssafibayNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Lesson Plan On RhinitisDocument15 pagesLesson Plan On Rhinitiskiran mahal100% (4)
- NCM107 - Midterm - Newborn CareDocument6 pagesNCM107 - Midterm - Newborn CareLjc JaslinNo ratings yet
- A Presentation On Pantothenic Acid or b5Document28 pagesA Presentation On Pantothenic Acid or b5jainsaketNo ratings yet
- Pedia Pulmo 2 10.18.16Document73 pagesPedia Pulmo 2 10.18.16Medisina101No ratings yet
- Bioactive Lipid Mediators - (2015)Document424 pagesBioactive Lipid Mediators - (2015)MohammedAjebliNo ratings yet
- PsychSim 5 Quizzing - Chapter 6-Sensation and PerceptionDocument5 pagesPsychSim 5 Quizzing - Chapter 6-Sensation and Perceptionneecee126100% (1)
- Parasitology Lect. (4) : Preparation of Solutions For Wet MountDocument5 pagesParasitology Lect. (4) : Preparation of Solutions For Wet MountAbdul hadiNo ratings yet
- Neuropathic Painn PDFDocument20 pagesNeuropathic Painn PDFkaktusNo ratings yet
- DR Anu Arasu How Trauma Affects Your HormonesDocument14 pagesDR Anu Arasu How Trauma Affects Your HormonesShalu SaharanNo ratings yet
- Amphibian Graphs?Document9 pagesAmphibian Graphs?Anshumaan PatraNo ratings yet
- Rubins-Q A ENDOCRINEDocument14 pagesRubins-Q A ENDOCRINECRUZ Jill EraNo ratings yet
- Newborn Hypothermia and Hyperthermia (Final Copy)Document30 pagesNewborn Hypothermia and Hyperthermia (Final Copy)Shizuka Marycris Amane67% (3)
- Case StudyDocument19 pagesCase StudyChristine MccombsNo ratings yet
- 29 Neuron Structure-SDocument6 pages29 Neuron Structure-SGrace MasseyNo ratings yet
- Liver Cirrhosis NCP 1Document6 pagesLiver Cirrhosis NCP 1Paolo Rafael D EsguerraNo ratings yet
- The TongueDocument21 pagesThe Tonguemanojchouhan2014No ratings yet
- Ppe4 Reflection AssignmentDocument11 pagesPpe4 Reflection Assignmentapi-318846856100% (1)
- The Pathophysiology of AmenorrheaDocument6 pagesThe Pathophysiology of AmenorrheaTri Suci UtamiNo ratings yet
- Sordaria Lab Written Assignment 1Document9 pagesSordaria Lab Written Assignment 1api-285000182100% (1)
- BTL Ultrasound 5000 - User ManualDocument16 pagesBTL Ultrasound 5000 - User ManualAlexaNo ratings yet
- Tissue Procurement, Processing, and Staining TechniquesDocument10 pagesTissue Procurement, Processing, and Staining TechniquesMuhammad JameelNo ratings yet
- 0 MnemonicsDocument133 pages0 MnemonicsAlex Ivan Chen TejadaNo ratings yet
- Cell Biology Test - 70 Possible Points: Prokaryotic and Eukaryotic Cells (2 Points Per Question)Document3 pagesCell Biology Test - 70 Possible Points: Prokaryotic and Eukaryotic Cells (2 Points Per Question)Vienne MonroidNo ratings yet
- 100 Benefits of ExerciseDocument3 pages100 Benefits of ExercisePaul RavenWolf JuniorNo ratings yet
- 英文TG900series 8885 lowDocument4 pages英文TG900series 8885 lowJose L GuzCamNo ratings yet
- X - Problem Prioritization and NCPDocument5 pagesX - Problem Prioritization and NCPMartin Lєtmaku Espina100% (2)
- Throwing RehabDocument16 pagesThrowing RehabSean GlynnNo ratings yet
- Week 006 Animal-Immune-SystemDocument13 pagesWeek 006 Animal-Immune-SystemMark Lorens StaanaNo ratings yet
- NCPDocument10 pagesNCPbabycheska08No ratings yet
- 5096 w09 Ms 2Document7 pages5096 w09 Ms 2Asiff MohammedNo ratings yet