You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pleural Disorders: 5/29/2018 1 by Shegaw Z (MSC in Ahn)Document61 pagesPleural Disorders: 5/29/2018 1 by Shegaw Z (MSC in Ahn)Amanuel MaruNo ratings yet
- Intoduction To Clinical NursingDocument58 pagesIntoduction To Clinical NursingAmanuel MaruNo ratings yet
- 2 Cholinergic BlockersDocument49 pages2 Cholinergic BlockersAmanuel MaruNo ratings yet
- c03 PDFDocument6 pagesc03 PDFUloko ChristopherNo ratings yet
- MicrobiologyDocument81 pagesMicrobiologyAmanuel MaruNo ratings yet
- 26 Biology 2 - 16 - 08 Cellular RespirationDocument48 pages26 Biology 2 - 16 - 08 Cellular RespirationAmanuel MaruNo ratings yet
- Introduction To Medical Surgical NursingDocument42 pagesIntroduction To Medical Surgical NursingAmanuel MaruNo ratings yet
- Laboratory Diagnosis of Parasitic DiseasesDocument57 pagesLaboratory Diagnosis of Parasitic DiseasesAmanuel MaruNo ratings yet
- 1.household Water Supply and Basic SanitationDocument8 pages1.household Water Supply and Basic SanitationAmanuel MaruNo ratings yet
- 856 3443 1 PB PDFDocument9 pages856 3443 1 PB PDFAmanuel MaruNo ratings yet
- Basic Concepts of Computer (1.25 MB)Document32 pagesBasic Concepts of Computer (1.25 MB)abhi_txt90No ratings yet
- ICTFactsFigures2016 PDFDocument8 pagesICTFactsFigures2016 PDFPaulo HenriqueNo ratings yet
- PartyooDocument1 pagePartyooAmanuel MaruNo ratings yet
- Tayangan Organisasi Komputer D3 - TKDocument358 pagesTayangan Organisasi Komputer D3 - TKMelkie WalelignNo ratings yet
- Ch.01 Introduction To ComputersDocument10 pagesCh.01 Introduction To ComputersSam Daka100% (1)
- Chapter III Gram Positive RodsDocument70 pagesChapter III Gram Positive RodsAmanuel MaruNo ratings yet
- Health & Human BehaviorDocument56 pagesHealth & Human BehaviorAmanuel Maru100% (2)
- Computer-Basics - Computer Basics2Document43 pagesComputer-Basics - Computer Basics2api-216226726No ratings yet
- Introduction To ComputingDocument270 pagesIntroduction To ComputingNadaNo ratings yet
- Revision Resources s4-6Document11 pagesRevision Resources s4-6Amanuel MaruNo ratings yet
- General PathologyDocument261 pagesGeneral PathologyHanif SharNo ratings yet
- 1,227 Qi FactsDocument14 pages1,227 Qi FactsMithilesh SinghNo ratings yet
- Day 3Document75 pagesDay 3Amanuel MaruNo ratings yet
- GT PharmacodynamicsDocument280 pagesGT PharmacodynamicsAmanuel MaruNo ratings yet
- Biochemistry of Red Blood Cells (Erythrocytes) - : Rajesh.P. NarayananDocument80 pagesBiochemistry of Red Blood Cells (Erythrocytes) - : Rajesh.P. NarayananAmanuel MaruNo ratings yet
- Ajbms 2011 2 08Document11 pagesAjbms 2011 2 08Amanuel MaruNo ratings yet
- Unit 1Document66 pagesUnit 1Amanuel MaruNo ratings yet
- For PC-I Medicine Students By: Zelalem ADocument39 pagesFor PC-I Medicine Students By: Zelalem AAmanuel MaruNo ratings yet
- LeukemiaDocument42 pagesLeukemiaAmanuel MaruNo ratings yet
- Bioch - of RBC CompleteDocument88 pagesBioch - of RBC CompleteAmanuel MaruNo ratings yet
- Asd ClosureDocument1 pageAsd ClosureEndy Widya PutrantoNo ratings yet
- Multiple-Choice Questions Cardiology Questions For (UK) : The MRCP ExaminationDocument6 pagesMultiple-Choice Questions Cardiology Questions For (UK) : The MRCP ExaminationDr.vidyaNo ratings yet
- Exercise Tolerance TestDocument15 pagesExercise Tolerance TestahmedNo ratings yet
- New-Onset Atrial Fibrillation in The Post-Primary Pci Setting: A Systematic ReviewDocument9 pagesNew-Onset Atrial Fibrillation in The Post-Primary Pci Setting: A Systematic ReviewTeodorNo ratings yet
- Novilyn C. Pataray BSN - Ii: Assessment Diagnosis Pathophysiolog Y Planning Intervention Rationale EvaluationDocument1 pageNovilyn C. Pataray BSN - Ii: Assessment Diagnosis Pathophysiolog Y Planning Intervention Rationale EvaluationCharina Aubrey100% (3)
- ValvopatiasDocument97 pagesValvopatiasapi-3826574No ratings yet
- Hridroga SampraptiDocument39 pagesHridroga SampraptiGAURAVNo ratings yet
- Valvular Heart Disease 2Document46 pagesValvular Heart Disease 2Topea BogdanNo ratings yet
- Echo Pocket 2014Document18 pagesEcho Pocket 2014abbouamine100% (2)
- Ritter RulesDocument1 pageRitter RulesSunny NgNo ratings yet
- LITFL - Wellens SyndromeDocument8 pagesLITFL - Wellens Syndromesunil abrahamNo ratings yet
- Kontribusi Hipertensi Dan Diabetes Mellitus Tipe 2 Atau Keduanya Terhadap Stroke BerulangDocument7 pagesKontribusi Hipertensi Dan Diabetes Mellitus Tipe 2 Atau Keduanya Terhadap Stroke BerulangyolaNo ratings yet
- Acs TrombolitikDocument55 pagesAcs TrombolitikDiana IswardhaniNo ratings yet
- Mitral Stenosis Summary Notes PDFDocument5 pagesMitral Stenosis Summary Notes PDFCristina Georgiana CoticăNo ratings yet
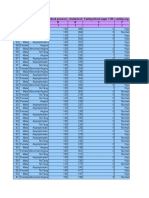
- Age Sex Chest Pain Type Blood Pressure Cholesterol Fasting Blood Sugar 120 Resting Ecg R C C R R C C I I I I I I IDocument14 pagesAge Sex Chest Pain Type Blood Pressure Cholesterol Fasting Blood Sugar 120 Resting Ecg R C C R R C C I I I I I I Isantu4_1111No ratings yet
- A. FlutterDocument8 pagesA. FlutterAdam ChungNo ratings yet
- What Is Hypertensive Heart DiseaseDocument11 pagesWhat Is Hypertensive Heart DiseaseamiraNo ratings yet
- Lecture On Heart Sounds by Dr. RoomiDocument15 pagesLecture On Heart Sounds by Dr. RoomiMudassar Roomi100% (1)
- Carotid Sinus MassageDocument3 pagesCarotid Sinus MassageSandeep m rNo ratings yet
- Crochetage' Sign On ECG in Secundum ASDDocument2 pagesCrochetage' Sign On ECG in Secundum ASDAishah Shalimar PutriNo ratings yet
- 500 Single Best Answers in MedicineDocument443 pages500 Single Best Answers in MedicineOmar Ahmed100% (1)
- ECG in Cardiac ChannelopathiesDocument37 pagesECG in Cardiac ChannelopathiesCarissa CkNo ratings yet
- Delta Wave - LITFL Medical Blog - ECG Library BasicsDocument9 pagesDelta Wave - LITFL Medical Blog - ECG Library BasicsLauraNo ratings yet
- Braunwald - UA and NSTEMIDocument49 pagesBraunwald - UA and NSTEMIusfcards100% (2)
- Heart AssessmentDocument7 pagesHeart AssessmentKinn Noha100% (1)
- Stroke and Cerebrovascular DiseaseDocument14 pagesStroke and Cerebrovascular DiseaseMarwan M.No ratings yet
- Pulmonary StenosisDocument19 pagesPulmonary StenosisAbdur RaqibNo ratings yet
- Xavier University-Ateneo de CagayanDocument3 pagesXavier University-Ateneo de CagayanMariano MarbellaNo ratings yet
- NCM116 Module 3 Cerebrovascular Disease QuizDocument5 pagesNCM116 Module 3 Cerebrovascular Disease QuizIvan FernandezNo ratings yet
- Medico Graph I A 128Document97 pagesMedico Graph I A 128Rafael CastilloNo ratings yet