Professional Documents
Culture Documents
Typhoid Journal1
Uploaded by
Riany Jade SabrinaCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Typhoid Journal1
Uploaded by
Riany Jade SabrinaCopyright:
Available Formats
Seminar
Typhoid fever
John Wain, Rene S Hendriksen, Matthew L Mikoleit, Karen H Keddy, R Leon Ochiai
Control of typhoid fever relies on clinical information, diagnosis, and an understanding for the epidemiology of the Published Online
disease. Despite the breadth of work done so far, much is not known about the biology of this human-adapted bacterial October 21, 2014
http://dx.doi.org/10.1016/
pathogen and the complexity of the disease in endemic areas, especially those in Africa. The main barriers to control S0140-6736(13)62708-7
are vaccines that are not immunogenic in very young children and the development of multidrug resistance, which Norwich Medical School,
threatens ecacy of antimicrobial chemotherapy. Clinicians, microbiologists, and epidemiologists worldwide need to University of East Anglia,
be familiar with shifting trends in enteric fever. This knowledge is crucial, both to control the disease and to manage Norwich, UK (Prof J Wain PhD);
cases. Additionally, salmonella serovars that cause human infection can change over time and location. In areas of National Food Institute,
Technical University of
Asia, multidrug-resistant Salmonella enterica serovar Typhi (S Typhi) has been the main cause of enteric fever, but Denmark, WHO Collaborating
now S Typhi is being displaced by infections with drug-resistant S enterica serovar Paratyphi A. New conjugate Centre for Antimicrobial
vaccines are imminent and new treatments have been promised, but the engagement of local medical and public Resistance in Foodborne
health institutions in endemic areas is needed to allow surveillance and to implement control measures. Pathogens and European
Union Reference Laboratory for
Antimicrobial Resistance,
Introduction Genomics of S Typhi Kongens Lyngby, Denmark
Estimates of disease burden Despite the genetic similarity of S Typhi and S enterica (R S Hendriksen PhD); National
Knowledge of the burden of disease is crucial for serovar Typhimurium (90% of genes are shared), Enteric Reference Laboratory
Team, Enteric Diseases
several reasonsfirst, data for eects of the disease on understanding is poor for the genetic dierences that Laboratory Branch, Centers for
human health and the local economy are essential to underlie the ability of S Typhi, but not S Typhimurium, Disease Control and
inform decision-makers in public health; second, to cause enteric fever.15 Large-scale transposon knockout Prevention, Atlanta, GA, USA
information about local trends is necessary to allocate libraries16 allow researchers to assess function at the (M L Mikoleit MASCP); Centre
for Enteric Diseases, National
resources; and third, understanding of local and genome level and show dierences between S Typhi Institute for Communicable
regional disease trends is needed to provide informed and S Typhimurium.17 The same genes in S Typhi and Diseases, Division in the
guidance to travellers. Global estimates for the burden S Typhimurium might have dierent regulatory National Health Laboratory
Service (NHLS), Johannesburg,
of typhoid fever (defined as symptomatic infection with pathways and possibly dierent functions.18 This
South Africa
S Typhi) are published regularly (269 million cases of exciting new technology might provide targets for (K H Keddy MBBCh, MMed);
typhoid fever were reported in 20101) and general vaccine development and new antibacterial drugs for Faculty of Health Sciences,
mortality data are available from global and regional S Typhi in endemic regions. The investigation of why University of the
Witwatersrand, Johannesburg,
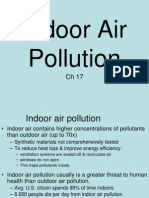
mortality studies (figure 1).2 However, detailed local S Typhi infects human beings, but not mice, has led to
South Africa (K H Keddy); and
surveillance data from endemic regions remain poor. the development of two mouse-studies for typhoid Independent Consultant
In this article, we provide an update on the previous fever: one is based on mice grafted with human (Vaccines), Tokyo, Japan
Seminar by providing an update on information on haemopoietic stem cells19 and the other is based on (R L Ochiai DPhil)
typhoid fever in endemic regions of the world. mice grafted with bacterial flagella recognition cells Correspondence to:
Prof John Wain, Innovation
with Toll-like receptor-11 knockouts.20 Research has also
Centre, Norwich Research Park,
Diagnosis and treatment of typhoid fever led to the description of gtgE, a virulence gene present Norwich NR4 7GJ, UK
Recent reviews of diagnosis and treatment of typhoid in S Typhimurium but not in S Typhi that allows j.wain@uea.ac.uk
fever3,4 make it clear that the laboratory diagnosis of S Typhi to infect mouse macrophages. Although still to
typhoid fever is largely dependent on the detection be verified, these models could allow the previously
of organisms in blood by PCR (best suited to impossible investigation of pathogenesis and immunity
epidemiological surveys) or culture (although for this human-restricted pathogen. The importance of
sensitivity remains a limitation).46 The Widal test for these new models is shown by the use of the humanised
antibody production is unreliable and new-generation mouse model to describe receptor-binding specificity
serology tests such as typhidot and tubex have not and delivery mechanisms for the typhoid toxin encoded
proved reliable in Africa79 or Asia.10,11 One new test by ctdB and pltA21 and so to define a potential new
format that shows promise is the typhoidparatyphoid vaccine target.
diagnostic assay,12 which detects IgA. This method has
specificity of detection of circulating IgA for the Search strategy and selection criteria
diagnosis of typhoid fever with use of ELISA11 and We searched PubMed and Web of Knowledge for articles
improves the sensitivity (to 100%) through published in English from Jan 1, 2008, to Dec 31, 2013, using
amplification of the signal by isolation and incubation the terms typhoid or Typhi. We did searches for highly
of peripheral blood lymphocytes.13 Treatment with cited articles in Web of Knowledge and Google Scholar that
fluoroquinolones, azithromycin, and third-generation were tracked for citations since Jan 1, 2008. We also used the
cephalosporin drugs is the main treatment, with contacts and experience of the authors who live and work
chloramphenicol used in regions in which susceptible across the typhoid endemic regions of Asia and Africa.
strains are present (panel 1).8
www.thelancet.com Published online October 21, 2014 http://dx.doi.org/10.1016/S0140-6736(13)62708-7 1
Seminar
A Female individuals B Male individuals
Hepatitis Poisonings Trachea, bronchus and lung Fire, heat, and Poisonings Hepatitis 11%
Drowning 12% 09% hot substances 12% Typhoid and
cancers
09% 12% CKD paratyphoid fevers
Diabetes 11% Diabetes
CKD 11% 09%
Chronic 14% Other non-communicable 11%
respiratory 14% Breast and cervical cancer diseases Falls Nutritional
diseases 21% 42% 20% 18% deficiencies
Diarrhoeal diseases 08%
Typhoid and
paratyphoid fevers 19%
Drowning
11% 20% Cardiovascular
Digestive diseases HIV/AIDS Chronic respiratory diseases disease
and cirrhosis 144% 21% Digestive diseases 128%
38% Nutritional (except cirrhosis)
deficiencies Maternal 21% Malaria Road injury
17% disorders
23% 107%
73%
Interpersonal violence Other communicable,
16% maternal, neonatal, and
Other
Lower respiratory non-communicable nutritional conditions
infections Diarrhoea diseases 26% HIV/AIDS
32% 118% 107%
28% Lower Cirrhosis
Neurological or mental respiratory of the liver
and behavioural infections 36%
Cardiovascular 28%
disorders 30% disease
Other Neurological or mental Neoplasms
Other communicable, 107%
injuries and behavioural disorders Other 94%
maternal, neonatal, injuries
75% 35% Self-harm
and nutritional 62%
Malaria 57%
conditions Tuberculosis
28%
27% 51%
Fire, heat, and Interpersonal
hot substances Road injury Tuberculosis Self-harm violence
26% 05% 46% 48% 52%
Figure 1: Mortality from enteric fever worldwide
Data from Jan 1, 2012, to Dec 31, 2012. 5 741 344 total deaths. CKD=chronic kidney disease. Used from Lozano and colleagues.2
Typhoid fever in Asia
Panel 1: Key issues in diagnosis and treatment of typhoid Data from global burden of disease studies show most
in developing countries cases of typhoid fever to be reported on the Indian
Emphasis should be placed on disease prevention; subcontinent;1,22,23 however disease burden is not uniform
short-term measures include vaccination of high-risk within this region (table 1). In addition to variation by
populations in endemic areas, and rational and judicious location and age group, dierences are also noted in
antibiotic drug prescribing practices by health incidence of typhoid fever over time in one location.
professionals Retrospective analysis of data for Salmonella spp infection
In endemic regions, diagnostics do not meet the daily from an urban hospital in Kathmandu, Nepal, shows an
challenge of dierentiation of the causes of fever and the increase in typhoid fever as cause of community acquired
disease burden for enteric fever cannot be defined septicaemia. Among 82 467 blood cultures done,
Development of new diagnostic tests is a challenge Salmonella spp accounted for 75%28 of positive cultures, of
because of low numbers of bacteria in the blood and which 71% (9124) tested positive for S Typhi. Between
antigenic cross-reactivity with other Gram-negative 19972000 and 200103, Salmonella spp septicaemia rates
bacteria significantly increased from 6% to 14%. Conversely,
New technologies to exploit the in-vivo induction of decreases in typhoid fever incidence have been reported in
antigens, immunoanity proteomics, and detection of the Mekong Delta region and in southern China.2935
metabolic products could identify new diagnostic targets Southern China is of particular interest because the once
Outbreaks of multidrug-resistant typhoid fever need dominant S Typhi infection has now been replaced by
costly and widely unavailable drugs for eective treatment infection with S Paratyphi A.32 Although done with use of
There are no guidelines for the treatment of patients with suitable surveillance systems, including diagnosis by
quinolone-resistant S Typhi strains blood culture, the studies that we describe above were not
The lack of an adequate gold standard is a major standardised, which might bias comparisons between
hindrance in the development of new diagnostics for regionseg, incidence rate estimates are higher from
enteric fever and increases the size and cost of trials studies with active,2426 as compared with passive,
Adapted from Parry and colleagues4 and Zaki and colleagues14
surveillance studies.36 To address this comparability issue,
the International Vaccine Institute in Korea did several
2 www.thelancet.com Published online October 21, 2014 http://dx.doi.org/10.1016/S0140-6736(13)62708-7
Seminar
large studies that collected prospective population-based
Study design Incidence of typhoid fever
surveillance data in five Asian countries with use of
standardised surveillance, clinical, and microbiological Urban slums of Delhi24 Population based 98 per 1000 per year (3 times higher in children
(1820 people) younger than 5 years)
methods (table 2).36 The results confirm variation in
Urban slums in Household based 187 per 1000 per year in preschool-aged children;
distribution of typhoid fever. Overall incidence was Bangladesh25,26 (roughly 11 400 people) 21 per 1000 per year in older patients
1708 cases per 100 000 people per year, but this rate varied Coastal community in Household based 41 per 1000 per year in children younger than 5 years;
substantially from location to location. Even when broken Pakistan27 (5700 people) 44 per 1000 per year in children younger than 2 years
down by age group, variation in the annual typhoid
Preschool age usually indicates children aged 15 years.
fever incidence was still apparentfor children aged
2460 months: 5732 per 100 000 in Pakistan, Table 1: Estimations for burden of typhoid fever for regions within the Indian subcontinent
3401 per 100 000 in India, and 1487 per 100 000 in
Indonesia. These dierences are also shown in risk factors
Site Incidence of typhoid fever
across all sites. Consumption of water at work site,37
non-boiled untreated spring water,3840 water from a China Urban and rural 153 cases per 100 000 per year in people
aged 560 years old
non-municipal source,41 and contaminated tap water42 all
Vietnam Urban 242 cases per 100 000 per year in people
relate to waterborne transmission; whereas consumption aged 618 years old
of ice cream37 and consumption of food from outdoor Indonesia Urban slum 817 cases per 100 000 per year (all ages)
vendors37,43,44 suggest foodborne infection. There are also Pakistan Urban slum 4517 cases per 100 000 per year in
general risk factorsie, high population density,38,42 children aged 215 years
unsanitary living conditions,42 poor hygiene and hygiene India Urban slum 4935 cases per 100 000 per year
practices,41,43 low socioeconomic status,45 and recent contact (all ages)
with a patient with typhoid fever.45 Control measures
441 435 people in the targeted age groups were under surveillance for 1 year at
should be tailored to local data, which are not available. each site (the 12 month period was between August 2002 and July 2004).
463 culture-confirmed cases of typhoid fever were described.36
Typhoid fever in Africa Table 2: Surveillance data from sites in five Asian countries
Typhoid fever is even less well understood in Africa than it
is in Asia; largely due to poor resources for laboratory
diagnostics and insucient infrastructure to support acknowledged in Kenya in 2009, where investigators
epidemiological and clinical studies. These problems are identified the need to establish better estimates of the
manifestations of the challenges faced by a large, largely disease burden.50 One method to address this issue could
impoverished, continent with a high burden of HIV and be to use local resources; several facilities in the least
unstable governments and with health-care priorities that developed regions of Africa are capable of laboratory-based
overwhelm a countrys ability to provide safe food and studies and have contributed to data for the disease, again
potable water. In Africa, access to safe water should not be results show large regional variation.
confused with access to piped water because water Comparison between surveillance data for Malawi and
treatment plants age and resources are diminished.46 South Africa shows variance in demographics of patients
Attempts to define the burden of typhoid fever in Africa with typhoid fever. Typhoid fever in Malawi and
show very clearly a need for well designed studies. Crump South Africa remains a disease mainly in children aged
and colleagues23 attempted to calculate burden using 515 years,51 whereas in urban areas of Kenya (where
published studies and concluded that information was too crude incidence rates for typhoid fever can be as high as
scarce to estimate anything better than a crude incidence 247 cases per 100 000), disease is recorded predominantly
rate50 cases per 100 000 for a population of about in children younger than 10 years.52 Incidence in urban
820 million. The 2010 Global Burden of Disease study2 areas is 15 times that reported for rural Kenya.47 By
estimated similar rates, but Buckle and colleagues1 contrast, in Ghana the disease seems to be more common
increased these estimates7246 cases per 100 000with in children younger than 5 years,53 and in Moshi, Tanzania,
the addition of rates from one publication from Kenya.47 typhoid fever is commonly diagnosed in both adults and
The dierence in estimates is driven by data from an area children.54,55 These data, as with the early data from Asia,
in which no interventions to control typhoid fever had are not comparable, but clearly there are huge
been introduced. Earlier studies, as used by Crump and demographic and geographic dierences in individuals
colleagues,23 assessed typhoid fever incidence rates after who are susceptible to typhoid fever. The situation in
two large placebo-controlled trials for the typhoid vaccine. Zimbabwe is of particular concernthe ocial
These trials involved more than 11 000 people in cumulative figures for 2013 to the end of April report more
South Africa48 and more than 32 000 people in Egypt49 and than 6800 suspected disease cases and 142 patients
so herd immunity (and hence decreasing incidence of confirmed to have typhoid fever.56
typhoid fever in the controls) might have lowered disease A confounding factor in estimation of burden for
rates. The shortcomings in use of these data for a continent typhoid fever is the rise of non-typhoidal salmonellosis
of 1045 million people that covers 303 million km were as an invasive and often fatal disease in Africa (table 3);57
www.thelancet.com Published online October 21, 2014 http://dx.doi.org/10.1016/S0140-6736(13)62708-7 3
Seminar
in Africa61 and sporadic cases associated with travel to an
Findings
African country,6164 although these reports are less frequent
Moshi, Tanzania54,55 Typhoid fever is more common than is non-typhoidal salmonellosis in both than are reports of typhoid fever associated with travel to
children and adults
Asia.62,65,66 The threat of invasive, multidrug-resistant
Malawi and South Africa51 Typhoid fever seen mainly in children aged 515 years with a case frequency
lower than that for non-typhoidal salmonellosis organisms circulating in a region with little capacity for
Kenya52 Typhoid fever more common than non-typhoidal salmonellosis in an urban area epidemiology and laboratory study show the need for
Pemba Island, Tanzania59 Salmonella enterica serovar Typhi is the most prevalent isolate from blood cultures
international collaboration and standardised methods to
Lagos, Nigeria7 Salmonella enterica serovar Typhi the most common Salmonella spp in blood
identify and subtype these pathogens. We are aware of
cultures (19992008); estimated incidence 16 cases per 100 000 some initiativeseg, WHO supports an external quality
assessment programme through its Regional Oce for
Table 3: Comparison of typhoid fever with non-typhoidal salmonellosis Africa, and the WHO Global Foodborne Infections
Network oers training and simplified biochemical
this issue has not been reported in Asia.58 A lack of procedures for identification of Salmonella spp (including
appropriate technology for Salmonella spp serotyping in S Typhi) and Shigella spp (panel 2). International
For more on PulseNet see low-resource settings prevents discrimination between collaboration between participants of PulseNet have
http://www.cdc.gov/pulsenet/ enteric fever caused by S Typhi or S Paratyphi A and tracked isolates (and patients) across continents;61
infection with non-typhoidal salmonellosis, therefore investigations that were enhanced by laboratories in Africa.
rates might obscure the true incidence of typhoid fever. In summary, much is not known about typhoid fever in
Control measures, such as prevention with vaccination, Africa; and appropriate technology to assess the actual
treatment with antibacterial drugs, and control of burden of disease is not available.8 Very little is known
transmission with public health interventions, are about the apparent protective eect of HIV against typhoid
dierent for invasive non-typhoidal salmonellosis, fever,54,55 the role of vertical transmission, and the potential
typhoid fever, and paratyphoid fever; therefore, it is eect of inclusion of typhoid fever in a dierential
important that all of these diseases are recognised. diagnosis in neonatal sepsis in endemic areas;67 the role of
A further threat to control of typhoid fever in Africa, as outbreaks of circulating endemic strains in the generation
it is elsewhere, is that of multidrug resistance. Culture of population immunity in all people apart from very
remains the preferred method to confirm cases of young children;60 the role of strain variation in outbreaks
typhoid fever and to capture information about emerging with high mortality rates that are complicated by intestinal
antimicrobial resistance in S Typhi in Africa. However, in perforation68 (or neurological manifestations69); and the
outbreaks, the newer rapid diagnostic tests, although not role of contaminated water supplies.70 Diagnosis and
ideal, might be more useful than culture to define the management of typhoid fever in Africa is aected by
extent of the outbreak.710 These tests cannot replace several challenges, including poor access to epidemiological
culture and recommendations for locations with poor and diagnostic resources, inadequate supply of safe water
resources are to continue culture of certain patients so and sanitation, and rapidly emerging resistance to
that data for antimicrobial susceptibility are recorded. antimicrobial drugs. Concerted eorts through provision
Although it is rare to find a documented travel history for of safe food and water and targeted vaccination
African patients, most multidrug-resistant cases of typhoid campaigns7173 could help to control typhoid fever in Africa.
fever in Africa seem to be mainly from outside the
continent.60 Investigators have reported endemic outbreaks Antimicrobial drug resistance
The global distribution of drug resistance in S Typhi
Mortality rates in patients with typhoid fever who are not
Panel 2: Training courses from the WHO Global Foodborne given specific chemotherapy can be as high as 26%,74
Infections Network although earlier work describes mortality rates of 10% or
For the WHO Global Foodborne The Global Foodborne Infections Network is a WHO network lower that were associated with careful management
Infections Network website see that among others builds capacity to detect, control, and including strict adherence to a milk diet.75 The
http://www.
prevent foodborne and other enteric infections. More than introduction of chloramphenicol (in 1948), ampicillin
antimicrobialresistance.dk/232- (1961), co-trimoxazole (1970s), and third-generation
169-215-protocols.htm 80 training courses are coordinated through Technical
University of Denmark, National Food Institute, Denmark, cephalosporins and fluoroquinolones (1980s) reduced
which is a WHO collaborating centre for antimicrobial the mortality of typhoid fever considerably. However,
resistance. Through this work, the institute is involved with multidrug-resistant strains14 that were resistant to all
surveillance of global antimicrobial resistance. Protocols three first-line antimicrobial drugs emerged in the 1980s,
that cover, among others, antimicrobial suscptibility testing, followed by stains resistant to fluoroquinolones in the
identification and isolation of foodborne pathogens, and 1990s.76,77 Cephalosporin resistance has been slower to
pulsed-field gel electrophoresis, and complete sets of emerge, but extended-spectrum -lactamase-producing
protocols for the dierent levels of training courses needed organisms are increasingly noted.78 If extended-spectrum
are on the website of the network. -lactamase-producing S Typhi become widespread,
then treatment options could become severely scarce.79
4 www.thelancet.com Published online October 21, 2014 http://dx.doi.org/10.1016/S0140-6736(13)62708-7
Seminar
Azithromycin is increasingly given for enteric fever, but isolates of S Typhi that were multidrug resistant. A few
is mainly used to treat children and patients with countries (Kuwait,85 Saudi Arabia,86 and Lebanon87) have
multidrug-resistant enteric fever because of its cost.80 reported detection of strains that were multidrug resistant
Salmonella spp breakpoints for azithromycin are not and had decreased ciprofloxacin susceptibility. From
formalised, complicating comparison with reported Kuwait there have also been reports of extended-spectrum
resistance; however the European Committee on beta-lactamase-producing S Typhi.88
Antibiotic Susceptibility Testing issued interpretative Substantial rates of resistance to first-line antimicrobial
criteria that regard susceptible S Typhi isolates as those drugs were detected in southeast Asia in the 1990s. This
with minimum inhibitory concentrations of 16 mg/L trend prompted authorities to change empirical
or lower. treatment guidelines for enteric fever from recom-
As long-distance travel becomes more accessible and mendations for chloramphenicol to recommendations
residents in developed countries visit friends and for fluoroquinolones. This change resulted in the
relatives in typhoid-endemic areas, health-care providers progressive re-emergence of susceptibility to first-line
in all countries need access to information about local drugs and a rapid increase in resistance to nalidixic acid.
and regional susceptibility to guide empirical treatment. For example, in Karnataka, India, 58% of S Typhi isolates
This need will remain until the development of rapid collected between 1996 and 1999 were multidrug
diagnostics that can predict the susceptibility to an resistant; whereas in 2004, no multidrug-resistant
infecting organism. Peer-reviewed data for antibiotic S Typhi isolates could be identified.89 In Nepal in 2006,
resistance of S Typhi in the Americas are extremely only 3% of isolates were classified as multidrug
scarce, but data available from regional laboratories81 and resistant.90 Investigators for a similar study in 2012 in
from investigation of travellers returning to the USA82 Nepal identified no ampicillin resistance in S Typhi.91
suggest little resistance in the region (figure 2). However, the global spread and clonal expansion of
In non-endemic Europe, 1417 confirmed cases of typhoid multidrug resistance and decreased ciprofloxacin
fever were reported to the European Centre for Disease susceptibility in clones suggests that this trend might
Prevention and Control in 2012, of which most cases were not last and that the reintroduction of previously used
either travel-related or in patients with an unknown travel drugs will probably not be useful. The situation is
history. In Russia and central Asia, data for antimicrobial similar in Cambodia, China, Hong Kong, Indonesia,
resistance in S Typhi are available only from Russia, which Malaysia, South Korea, and Vietnam.35,9296 Researchers of
reported no resistance to cephalosporin drugs in isolates, two studies have described low rates of resistance in Lao;
high rates of resistance to nalidixic acid (88% of isolates), 16% of the S Typhi isolates were multidrug resistant,
and moderate rates of resistance to other antimicrobial with no combined nalidixic acid resistance detected in
drug classes, including ciprofloxacin (2%) and nalidixic these strains.92,97 By contrast, two confirmed cases of
acid from 2005 to 2011 (figure 2).84 extended-spectrum -lactamase-producing S Typhi have
Most countries in the Middle East have reported detection been reported in the Philippines (figure 2).
of S Typhi strains with decreased ciprofloxacin susceptibility. In Africa, the emergence of S Typhi strains with
Several countries (Afghanistan, Jordan, Libya, Morocco, multidrug resistance7,47,98 and decreased ciprofloxacin
and the United Arab Emirates) have reported detection of susceptibility7,64,99102 is now an important issue. Rates of
Susceptible strains of S Typhi only present
MDR S Typhi present
Strains with combined MDR and decreased
susceptibility to ciprofloxacin present
ESBL-resistant S Typhi present
Typhoid-endemic countries with
insucient data available
Figure 2: Worldwide distribution of antimicrobial drug resistance in Salmonella enterica serovar Typhi
MDR is defined as resistance to the first-line antimicrobial drugs ampicillin, co-trimoxazole, and chloramphenicol. MDR=multi-drug resistant. ESBL=extended-spectrum
beta-lactamase-producer. Adapted from Bhan and colleagues,83 with data up to April, 2013.
www.thelancet.com Published online October 21, 2014 http://dx.doi.org/10.1016/S0140-6736(13)62708-7 5
Seminar
multidrug resistance varyeg, 30% in the Democratic and the UAE,88 Iraq,78 Pakistan,119 and the Phillippines.12 Of
Republic of the Congo,55 63% in Ghana,97 70% in those, only the cases from India (blaCTX-M-15)88 Iraq, India
Kenya,98 and 100% during an outbreak along the (blaCTX-M-15)78,120 and the Phillippines (blaSHV-12)12 have been
MalawiMozambique border.59 During a prolonged confirmed. The first case of an AmpC-producing S Typhi
outbreak in western Uganda, the percentage of was reported in 2009 in which S Typhi isolates with the
multidrug-resistant strains of S Typhi rapidly increased blaCMY-2 gene were isolated from an Indian child.118
from 5% in 2009 to 83% in 2011, and rates of resistance This finding is not suprising since third-generation
to nalidixic acid increased from 0% in 2009 to 6% in cephalosporins are now being given due to the wide
2011, and reached 875% in 2012.103 About 14% of isolates distribution of multidrug-resistant S Typhi isolates with
collected during 2011 in South Africa were nalidixic acid decreased cephalosporin susceptibility, and so selective
resistant, none of these isolates were resistant to pressure for resistance is increasing.
ceftriaxone or imipenem. The global spread of a resistant
strain, haplotype 58 (H58), described initially in Emerging resistance
southeast Asia101 and now present in Africa,60 is of Increasing isolate resistance to fluoroquinolones and
particular major concern and highlights a need to the emergence of cephalosporin resistance are of
improve epidemiological investigation to define the concern. Fourth-generation fluoroquinolones have good
origin of multidrug-resistant clones. activity against S Typhi, but concerns about toxic eects
(gatifloxacin was banned by the Indian Government in
Mobile genetic elements in S Typhi 2011), cross-resistance to other fluoroquinolones, and
The worldwide emergence of resistance to first-line stewardship initiatives (potentially limiting moxifloxacin
antibiotic drugs has been associated with a well described to treatment for tuberculosis121) could prevent the
group of plasmids, incHI1.104108 Occasionally, investigators widespread use of these drugs for typhoid fever.
have reported other plasmids in extended-spectrum Although not widely used, carbapenem drugs and
-lactamase-producing S Typhi, but occurrence is rare.104 tigecycline show good in-vitro activity and are potentially
Many of the resistance genes that cause the drugs of last resort.122 The re-emergence of strains
multidrug-resistance phenotype of S Typhi are contained susceptible to chloramphenicol and co-trimoxazole has
in incHI1 plasmids that contain several mobile elements raised the possibility of re-introduction of these first-line
(Tn9, Tn10, and Tn21), which, in turn, might contain antimicrobial drugs, but concerns remain that resistance
class one integrons.109 Some researchers have speculated would develop rapidly.79,101,123
that the presence of genes that encode resistance to
antimicrobial drugs and to heavy metals are maintained Vaccination
in the bacterial population through selective advantage Available vaccines
for plasmid carriage in S Typhi,109 and that this carriage At present, typhoid fever can be eectively treated with
led to the emergence of one plasmid type associated with antibiotic drugs, but the growing rates of antibiotic
a haplotype of S Typhi (H58).108 The next step in this rapid resistance make vital the consideration of a comprehensive
evolutionary pathway could be transfer of resistance approach to targeted vaccination of high-risk populations,
genes to chromosomes. combined with the longer-term solutions of provision of
safe water and improved sanitation. Vaccination against
Fluoroquinolone resistance in S Typhi S Typhi with heat-inactivated phenol-preserved, whole-cell
Fluoroquinolone resistance in Salmonella spp is usually typhoid is protective against typhoid fever; the vaccine has
mediated via chromosomal mutations, in the target 5188% ecacy in children and young adults, with
proteins, DNA gyrase (encoded by gyrA and gyrB), and protection for up to 7 years.124 Toxic eects led to
topoisomerase IV (parC and parE), or by plasmid-mediated development of new-generation vaccines in the 1970s
resistance, typically encoded on qnr or aac(6 )-Ib-cr. In one oral live attenuated vaccine (Ty21a) and one purified
S Typhi, increase in minimum inhibitory concentration Vi polysaccharide vaccine. The Ty21a vaccine three-dose
is associated with the accumulation of known regimen has an overall protective ecacy of between 67%
chromosomal mutations110114 including a novel mutation and 80%,125,126 but is only licensed for use in individuals
at codon 64 in gyrB.115 older than 2 years and availability is lower than needed.
As of August 2012, WHO is reviewing the application for
Extended-spectrum -lactamases in S Typhi prequalification of Ty21a to allow procurement through
Despite emerging resistance to extended spectrum UNICEF, the Pan American Health Organisation, and
cephalosporins and carbapenems in non-typhoidal other organisations such as GAVI Alliance.
salmonella in human beings and animals, not many cases The Vi vaccine was developed from virulent S Typhi
of extended-spectrum -lactamases in S Typhi have been with use of non-denaturing purification and elicits
reported. extended-spectrum cephalosporinase-producing anti-Vi serum IgG antibodies in 8595% of people older
strains of S Typhi have so far been reported only in than 2 years.127 The Vi vaccine is well tolerated, safe, and
sporadic cases in Bangladesh,116 Egypt,117 India,118 Kuwait shows evidence of herd protection when given to a large
6 www.thelancet.com Published online October 21, 2014 http://dx.doi.org/10.1016/S0140-6736(13)62708-7
Seminar
proportion of a community.128 The most common recently school-based pilots to introduce vaccine
side-eect is localised pain. Similar to other programmes with Vi polysaccharide have been done in
polysaccharide vaccines, Vi is not immunogenic in parts of Karachi, Pakistan, and Kathmandu, Nepal,
children younger than 2 years, and is licensed for use vaccinating nearly 400 000 students. In China, technology
from this age. There was no patent protection for the transfer by the US National Institutes of Health allowed
production technology of Vi vaccine so manufacturers six state-run vaccine companies to produce the vaccine
in developing countries began producing the vaccine in for the mass vaccination of school children and food
the 1990s. At present, at least 3 manufacturers export handlers in the mid-1990s. The Chinese programmes
the vaccine (Sanofi Pasteur, GlaxoSmithKline have largely reduced incidence of typhoid in some areas
Biologicals, and Bharat Biotech) and many other of southwest China (eg, parts of Guangxi32). The Vietnam
companies produce it for local use (eg, Lanzhou National Immunisation Programme also began annual
Institute in China, Chengdu Institute in China, Finlay campaigns in 1997 with use of imported and then
Institute in Cuba, and Dalat Vaccine Company in locally-produced Vi polysaccharide vaccines for children
Vietnam). WHO prequalified one of these vaccines, aged 310 years in some high-incidence districts.
from Sanofi Pasteur, and it is available to purchase for Although there is no data to assess its eect, Delhi state,
the UN agencies and the GAVI Alliance. India, introduced use of Vi polysaccharide vaccines in
children aged 25 years through community-based
Future vaccines vaccination campaigns in 2004. Thus, available vaccines
Vaccines are poorly immunogenic in young children are eective methods for public health, but are still not
and immunity lasts only a few years. The most accessible being used widely enough to protect whole populations.
vaccination route is to young children through the
expanded programme for immunisation and, in Conclusions
developing countries, young children are those who Typhoid fever remains the predominant enteric fever
probably have the highest burden of disease. There are worldwide, but enteric fever caused by S Paratyphi A is
therefore eorts to develop new vaccines that can be increasingly reported.35,135,136 Since the dierent Salmonella
given to young children. The most advanced is a spp serovars that cause enteric fever have very dierent
glycol-protein conjugated vaccine, the Vi-conjugate ancestries, clinical similarities must be the result of
vaccine. There are several dierent protein carriers to convergent evolution and it is therefore not appropriate to
the Vi-conjugate vaccinerecombinant exoprotein of assume that all enteric fever can be managed in the same
Pseudomonas aeruginosa (rEPA), tetanus toxoid, and way; risk factors vary,135 and vaccines are not cross-protective.
diphtheria toxoid or its derivative CRM197. Vi-rEPA was However, there is scope for a concerted disease-prevention
first developed by the US National Institutes of Health programme against all enteric fevers through use of
and underwent clinical trials in the USA and Vietnam, improved surveillance to dierentiate between the causes
but production was not brought forward to industrial of enteric fever so that public health interventions can be
scale.129 Two Vi-conjugate vaccines are licensed in targeted correctly and any further serovar replacement can
India, both conjugated to tetanus toxoid (PedaTyph be detected early. For the findings outlined in this Seminar
and TypBar-TCV). Other candidate Vi conjugate vaccines to be used, support for laboratories within developing
are in clinical trials done by several manufacturers and countries is essential.
developers,130,131 and single-dose live attenuated oral Contributors
vaccines, which could be given to infants, are in KHK did the searches for and wrote the section on typhoid fever in
development.132,133 Although research into novel vaccine Africa. MLM and RSH did the searches for and wrote the section on
antimicrobial resistance. RSH also created figure 2. JW drafted the
candidates rightly continues,21 implementation of outline for the original Seminar, recruited the authors, drafted the
existing vaccines is priority for global control of typhoid. general introduction and conclusions, created the reference list, did
the article coordination and final drafting, responded to the reviewers,
Programmatic use of vaccines and created figure 1 and the panels and tables. RLO did the searches
for and wrote the sections on typhoid fever in Asia and vaccination.
WHO recommended use of typhoid vaccines in high-risk All authors had input into final Seminar, including for revisions.
populations in 1999; however, the public sectors of only
Declaration of interests
three countries have complied.71,134 Use as a preventive KHK is a permanent employee of the National Institute for
action has been reportedie, after a tsunami in 2004, Communicable Diseases, South Africa. MLM is a permanent employee of
Pondicherry (India) local government used 17 000 doses the US Government (Department of Health and Human Services, Centers
of Vi polysaccharide vaccine; in 2010 after cyclone Tomas, for Disease Control and Prevention). The findings and conclusions in this
manuscript are those of the authors and do not necessarily represent the
the Vi polysaccharide vaccine was used as a response to ocial position of the Centers for Disease Control and Prevention. RSH
an outbreak of typhoid in Fiji to control the outbreak and is permanently employed by the Technical University of Denmark,
prevent further spread from the neighbouring villages; National Food Institute. JW is the Chief Scientific Ocer and Director for
in 2009 the Government of Sri Lanka set up a guideline Discuva, an antibiotic discovery company. RLO is currently an employee
of Sanofi Pasteur, which is a producer of typhoid vaccine. He was formerly
to vaccinate, with Vi polysaccharide vaccine, the internally an employee of the International Vaccine Institute, Seoul, Korea and
displaced population after the civil war; and more independent at the time of writing
www.thelancet.com Published online October 21, 2014 http://dx.doi.org/10.1016/S0140-6736(13)62708-7 7
Seminar
Acknowledgments 22 Bhutta ZA, Punjwani N, Lindblad BS. Concomitant bacteraemia as a
We thank the sta of the laboratories and hospitals that generated the risk factor for diarrhoeal disease mortality in Karachi: a case-control
data we report. study of hospitalized children. Acta Paediatr 1996; 85: 80913.
23 Crump JA, Luby SP, Mintz ED. The global burden of typhoid fever.
References Bull World Health Organ 2004; 82: 34653.
1 Buckle GC, Walker CL, Black RE. Typhoid fever and paratyphoid
fever: systematic review to estimate global morbidity and mortality 24 Sinha A, Sazawal S, Kumar R, et al. Typhoid fever in children aged
for 2010. J Glob Health 2012; 2: 10401. less than 5 years. Lancet 1999; 354: 73437.
2 Lozano R, Naghavi M, Foreman K, et al. Global and regional 25 Brooks WA, Hossain A, Goswami D, et al. Bacteremic typhoid fever
mortality from 235 causes of death for 20 age groups in 1990 and in children in an urban slum, Bangladesh. Emerg Infect Dis 2005;
2010: a systematic analysis for the Global Burden of Disease Study 11: 32629.
2010. Lancet 2012; 380: 2095128. 26 Naheed A, Ram PK, Brooks WA, et al. Burden of typhoid and
3 Khan KH. Recent trends in typhoid researchA Review. Int J Biosci paratyphoid fever in a densely populated urban community, Dhaka,
2012; 2: 11020. Bangladesh. Int J Infect Dis 2010; 14 (suppl 3): e9399.
4 Parry CM, Wijedoru L, Arjyal A, Baker S. The utility of diagnostic 27 Owais A, Sultana S, Zaman U, Rizvi A, Zaidi AK. Incidence of
tests for enteric fever in endemic locations. Expert Rev Anti Infect Ther typhoid bacteremia in infants and young children in southern
2011; 9: 71125. coastal Pakistan. Pediatr Infect Dis J 2010; 29: 103539.
5 Wain J, Hosoglu S. The laboratory diagnosis of enteric fever. 28 Maskey AP, Basnyat B, Thwaites GE, Campbell JI, Farrar JJ,
J Infect Dev Ctries 2008; 2: 42125. Zimmerman MD. Emerging trends in enteric fever in Nepal:
9124 cases confirmed by blood culture 19932003.
6 Baker S, Sarwar Y, Aziz H, et al. Detection of Vi-negative Trans R Soc Trop Med Hyg 2008; 102: 9195.
Salmonella enterica serovar Typhi in the peripheral blood of patients
with typhoid fever in the Faisalabad region of Pakistan. 29 Lin FY, Ho VA, Khiem HB, et al. The ecacy of a Salmonella typhi
J Clin Microbiol 2005; 43: 441825. Vi conjugate vaccine in two-to-five-year-old children. N Engl J Med
2001; 344: 126369.
7 Akinyemi KO, Oshundare YO, Oyeyinka OG, Coker AO.
A retrospective study of community-acquired salmonella infections 30 Lin FY, Vo AH, Phan VB, et al. The epidemiology of typhoid fever in
in patients attending public hospitals in Lagos, Nigeria. the Dong Thap Province, Mekong Delta region of Vietnam.
J Infect Dev Ctries 2012; 6: 38795. Am J Trop Med Hyg 2000; 62: 64448.
8 Keddy KH, Sooka A, Letsoalo ME, et al. Sensitivity and specificity of 31 Yang HH, Wu CG, Xie GZ, et al. Ecacy trial of Vi polysaccharide
typhoid fever rapid antibody tests for laboratory diagnosis at vaccine against typhoid fever in south-western China.
two sub-Saharan African sites. Bull World Health Organ 2011; Bull World Health Organ 2001; 79: 62531.
89: 64047. 32 Jin Y. Enteric fever in south China: Guangxi province.
9 Ley B, Thriemer K, Ame SM, et al. Assessment and comparative J Infect Dev Ctries 2008; 2: 28388.
analysis of a rapid diagnostic test (Tubex(R)) for the diagnosis of 33 Zhou WZ, Koo HW, Wang XY, et al. Revaccination with
typhoid fever among hospitalized children in rural Tanzania. locally-produced Vi typhoid polysaccharide vaccine among Chinese
BMC Infect Dis 2011; 11: 147. school-aged children: safety and immunogenicity findings.
10 Dutta S, Sur D, Manna B, et al. Evaluation of new-generation Pediatr Infect Dis J 2007; 26: 100105.
serologic tests for the diagnosis of typhoid fever: data from a 34 Nga TV, Parry CM, Le T, et al. The decline of typhoid and the rise of
community-based surveillance in Calcutta, India. non-typhoid salmonellae and fungal infections in a changing HIV
Diagn Microbiol Infect Dis 2006; 56: 35965. landscape: bloodstream infection trends over 15 years in southern
11 House D, Wain J, Ho VA, et al. Serology of typhoid fever in an area Vietnam. Trans R Soc Trop Med Hyg 2012; 106: 2634.
of endemicity and its relevance to diagnosis. J Clin Microbiol 2001; 35 Dong BQ, Yang J, Wang XY, et al. Trends and disease burden of
39: 100207. enteric fever in Guangxi province, China, 19942004.
12 Sheikh A, Bhuiyan MS, Khanam F, et al. Salmonella enterica serovar Bull World Health Organ 2010; 88: 68996.
Typhi-specific immunoglobulin A antibody responses in plasma 36 Ochiai RL, Acosta CJ, Danovaro-Holliday MC, et al, for the Domi
and antibody in lymphocyte supernatant specimens in Bangladeshi Typhoid Study Group. A study of typhoid fever in five Asian countries:
patients with suspected typhoid fever. Clin Vaccine Immunol 2009; disease burden and implications for controls. Bull World Health Organ
16: 158794. 2008; 86: 26068.
13 Khanam F, Sheikh A, Sayeed MA, et al. Evaluation of a typhoid/ 37 Luby SP, Faizan MK, Fisher-Hoch SP, et al. Risk factors for typhoid
paratyphoid diagnostic assay (TPTest) detecting anti-Salmonella IgA fever in an endemic setting, Karachi, Pakistan. Epidemiol Infect 1998;
in secretions of peripheral blood lymphocytes in patients in Dhaka, 120: 12938.
Bangladesh. PLoS Negl Trop Dis 2013; 7: e2316. 38 Khan MI, Ochiai RL, Soofi SB, et al. Risk factors associated with
14 Zaki SA, Karande S. Multidrug-resistant typhoid fever: a review. typhoid fever in children aged 216 years in Karachi, Pakistan.
J Infect Dev Ctries 2011; 5: 32437. Epidemiol Infect 2012; 140: 66572.
15 Sabbagh SC, Forest CG, Lepage C, Leclerc JM, Daigle F. So similar, 39 Mermin JH, Villar R, Carpenter J, et al. A massive epidemic of
yet so dierent: uncovering distinctive features in the genomes of multidrug-resistant typhoid fever in Tajikistan associated with
Salmonella enterica serovars Typhimurium and Typhi. consumption of municipal water. J Infect Dis 1999; 179: 141622.
FEMS Microbiol Lett 2010; 305: 113. 40 Swaddiwudhipong W, Kanlayanaphotporn J. A common-source
16 Langridge GC, Phan MD, Turner DJ, et al. Simultaneous assay of water-borne outbreak of multidrug-resistant typhoid fever in a rural
every Salmonella Typhi gene using one million transposon mutants. Thai community. J Med Assoc Thai 2001; 84: 151317.
Genome Res 2009; 19: 230816. 41 Gasem MH, Dolmans WM, Keuter MM, Djokomoeljanto RR.
17 Sabbagh SC, Lepage C, McClelland M, Daigle F. Selection of Poor food hygiene and housing as risk factors for typhoid fever in
Salmonella enterica serovar Typhi genes involved during interaction Semarang, Indonesia. Trop Med Int Health 2001; 6: 48490.
with human macrophages by screening of a transposon mutant 42 King CC, Chen CJ, You SL, Chuang YC, Huang HH, Tsai WC.
library. PLoS One 2012; 7: e36643. Community-wide epidemiological investigation of a typhoid
18 Barquist L, Langridge GC, Turner DJ, et al. A comparison of dense outbreak in a rural township in Taiwan, Republic of China.
transposon insertion libraries in the Salmonella serovars Typhi and Int J Epidemiol 1989; 18: 25460.
Typhimurium. Nucleic Acids Res 2013; 41: 454964. 43 Velema JP, van Wijnen G, Bult P, van Naerssen T, Jota S. Typhoid
19 Song J, Willinger T, Rongvaux A, et al. A mouse model for the fever in Ujung Pandang, Indonesiahigh-risk groups and high-risk
human pathogen Salmonella Typhi. Cell Host Microbe 2010; behaviours. Trop Med Int Health 1997; 2: 108894.
8: 36976. 44 Vollaard AM, Ali S, van Asten HA, et al. Risk factors for typhoid
20 Mathur R, Oh H, Zhang D, et al. A mouse model of Salmonella and paratyphoid fever in Jakarta, Indonesia. JAMA 2004;
typhi infection. Cell 2012; 151: 590602. 291: 260715.
21 Song J, Gao X, Galn JE. Structure and function of the 45 Luxemburger C, Chau MC, Mai NL, et al. Risk factors for typhoid
Salmonella Typhi chimaeric A(2)B(5) typhoid toxin. Nature 2013; fever in the Mekong delta, southern Viet Nam: a case-control study.
499: 35054. Trans R Soc Trop Med Hyg 2001; 95: 1923.
8 www.thelancet.com Published online October 21, 2014 http://dx.doi.org/10.1016/S0140-6736(13)62708-7
Seminar
46 Starkl M, Brunner N, Stenstrm TA. Why do water and sanitation 69 Lutterloh E, Likaka A, Sejvar J, et al. Multidrug-resistant typhoid
systems for the poor still fail? Policy analysis in economically fever with neurologic findings on the MalawiMozambique border.
advanced developing countries. Environ Sci Technol 2013; Clin Infect Dis 2012; 54: 110006.
47: 610210. 70 Centers for Disease Control and Prevention (CDC). Notes from the
47 Breiman RF, Cosmas L, Njuguna H, et al. Population-based field: Salmonella Typhi infections associated with contaminated
incidence of typhoid fever in an urban informal settlement and a waterZimbabwe, October 2011May 2012.
rural area in Kenya: implications for typhoid vaccine use in Africa. MMWR Morb Mortal Wkly Rep 2012; 61: 435.
PLoS One 2012; 7: e29119. 71 WHO. Position paper on typhoid vaccines. Wkly Epidemiol Rec 2008;
48 Klugman KP, Koornhof HJ, Robbins JB, Le Cam NN. 83: 4959.
Immunogenicity, ecacy and serological correlate of protection of 72 Hutton G. Global costs and benefits of reaching universal coverage
Salmonella typhi Vi capsular polysaccharide vaccine three years after of sanitation and drinking-water supply. J Water Health 2013; 11: 112.
immunization. Vaccine 1996; 14: 43538. 73 Kaljee LM, Pach A, Thriemer K, et al. Desirability for a typhoid
49 Wahdan MH, Sippel JE, Mikhail IA, et al. Controlled field trial of a fever vaccine among rural residents, Pemba Island, Tanzania.
typhoid vaccine prepared with a nonmotile mutant of Salmonella Vaccine 2013; 31: 299499.
typhi Ty2. Bull World Health Organ 1975; 52: 6973. 74 van den Bergh ET, Gasem MH, Keuter M, Dolmans MV. Outcome
50 Clemens JD. Meeting on establishment of consortium to study in three groups of patients with typhoid fever in Indonesia between
invasive Salmonelloses in Sub-Saharan Africa. Emerg Infect Dis 1948 and 1990. Trop Med Int Health 1999; 4: 21115.
2009; 15: e2. 75 Drigalski V. Ueber Ergebnisse bei der Bekampfung des Typhus
51 Feasey NA, Archer BN, Heyderman RS, et al. Typhoid fever and nach Robert Koch. ZBL Bakt Orign 1904; 35: 77698.
invasive nontyphoid salmonellosis, Malawi and South Africa. 76 Wain J, Hoa NT, Chinh NT, et al. Quinolone-resistant
Emerg Infect Dis 2010; 16: 144851. Salmonella typhi in Viet Nam: molecular basis of resistance and
52 Tabu C, Breiman RF, Ochieng B, et al. Diering burden and clinical response to treatment. Clin Infect Dis 1997; 25: 140410.
epidemiology of non-Typhi Salmonella bacteremia in rural and 77 Shetty AK, Shetty IN, Furtado ZV, Antony B, Boloor R. Antibiogram
urban Kenya, 20062009. PLoS One 2012; 7: e31237. of Salmonella isolates from blood with an emphasis on nalidixic acid
53 Marks F, Adu-Sarkodie Y, Hnger F, et al. Typhoid fever among and chloramphenicol susceptibility in a tertiary care hospital in
children, Ghana. Emerg Infect Dis 2010; 16: 179697. coastal Karnataka: a prospective study. J Lab Physicians 2012; 4: 7477.
54 Crump JA, Ramadhani HO, Morrissey AB, et al. Invasive bacterial 78 Pfeifer Y, Matten J, Rabsch W. Salmonella enterica serovar Typhi with
and fungal infections among hospitalized HIV-infected and CTX-M beta-lactamase, Germany. Emerg Infect Dis 2009; 15: 153335.
HIV-uninfected children and infants in northern Tanzania. 79 Kaurthe J. Increasing antimicrobial resistance and narrowing
Trop Med Int Health 2011; 16: 83037. therapeutics in typhoidal salmonellae. J Clin Diagn Res 2013; 7: 57679.
55 Crump JA, Ramadhani HO, Morrissey AB, et al. Invasive bacterial 80 Butler T. Treatment of typhoid fever in the 21st century: promises
and fungal infections among hospitalized HIV-infected and and shortcomings. Clin Microbiol Infect. 2011; 17: 95963.
HIV-uninfected adults and adolescents in northern Tanzania.
81 Cardona-Castro NM, Sanchez-Jimenez MM, Usuga-Silva LY, et al.
Clin Infect Dis 2011; 52: 34148.
Characterization of two typhoid fever outbreaks in Apartado,
56 ProMED. Typhoid fever update: Taiwan (ex Myanmar) Zimbabwe. Antioquia, 2005. Biomedica 2007; 27: 23643.
Mar 25. ProMED Digest 2013; 129.
82 Tatavarthy A, Sanderson R, Peak K, et al. Molecular typing and
57 Gordon MA. Invasive nontyphoidal Salmonella disease: epidemiology, resistance analysis of travel-associated Salmonella enterica serotype
pathogenesis and diagnosis. Curr Opin Infect Dis 2011; 24: 48489. Typhi. J Clin Microbiol 2012; 50: 263138.
58 Deen J, von Seidlein L, Andersen F, Elle N, White NJ, Lubell Y. 83 Bhan MK, Bahl R, Bhatnagar S. Typhoid and paratyphoid fever.
Community-acquired bacterial bloodstream infections in Lancet 2005; 366: 74962.
developing countries in south and southeast Asia: a systematic
84 Kovalenko AN, Zhdanov KV, Volzhanin VM, et al. Features of clinic,
review. Lancet Infect Dis 2012; 12: 48087.
diagnostics and treatment of typhoid fever in young patients.
59 Thriemer K, Ley B, Ame SS, et al. Clinical and epidemiological Voen Med Zh 2011; 332: 3339.
features of typhoid fever in Pemba, Zanzibar: assessment of the
85 Dimitrov T, Dashti AA, Albaksami O, Jadaon MM. Detection of
performance of the WHO case definitions. PLoS One 2012; 7: e51823.
mutations in the gyrA gene in fluoroquinolone resistance
60 Keddy KH, Sooka A, Ismail H, et al. Molecular epidemiological Salmonella enterica serotypes typhi and paratyphi A isolated from
investigation of a typhoid fever outbreak in South Africa, 2005: the the Infectious Diseases Hospital, Kuwait. J Clin Pathol 2010;
relationship to a previous epidemic in 1993. Epidemiol Infect 2011; 63: 8387.
139: 123945.
86 Somily AM, Sayyed SB, Habib HA, et al. Salmonella isolates
61 Smith AM, Keddy KH, Ismail H, et al, for the Group for Enteric, serotypes and susceptibility to commonly used drugs at a tertiary
Respiratory and Meningeal Disease Surveillance in South Africa care hospital in Riyadh, Saudi Arabia. J Infect Dev Ctries 2012;
(GERMS-SA). International collaboration tracks typhoid fever cases 6: 47882.
over two continents from South Africa to Australia. J Med Microbiol
87 Tohme A, Zein E, Nasnas R. Typhoid fever. Clinical and therapeutic
2011; 60: 140507.
study in 70 patients. J Med Liban 2004; 52: 7177.
62 Cooke FJ, Day M, Wain J, Ward LR, Threlfall EJ. Cases of typhoid
88 Rotimi VO, Jamal W, Pal T, Sovenned A, Albert MJ. Emergence of
fever imported into England, Scotland and Wales (20002003).
CTX-M-15 type extended-spectrum beta-lactamase-producing
Trans R Soc Trop Med Hyg 2007; 101: 398404.
Salmonella spp. in Kuwait and the United Arab Emirates.
63 Coovadia YM, Gathiram V, Bhamjee A, et al. The emergence of J Med Microbiol 2008; 57: 88186.
multi-antibiotic-resistant strains of Salmonella typhi in northern
89 Joshi S, Amarnath SK. Fluoroquinolone resistance in Salmonella typhi
Natal-KwaZulu. S Afr Med J 1992; 81: 28081.
and S paratyphi A in Bangalore, India. Trans R Soc Trop Med Hyg 2007;
64 Lunguya O, Lejon V, Phoba MF, et al. Salmonella typhi in the 101: 30810.
Democratic Republic of the Congo: fluoroquinolone decreased
90 Pokharel BM, Koirala J, Dahal RK, Mishra SK, Khadga PK,
susceptibility on the rise. PloS Negl Trop Dis 2012; 6: e1921.
Tuladhar NR. Multidrug-resistant and extended-spectrum
65 Lynch MF, Blanton EM, Bulens S, et al. Typhoid fever in the beta-lactamase (ESBL)-producing Salmonella enterica (serotypes Typhi
United States, 19992006. JAMA 2009; 302: 85965. and Paratyphi A) from blood isolates in Nepal: surveillance of resistance
66 Morita M, Hirose K, Takai N, et al. Salmonella enterica serovar Typhi and a search for newer alternatives. Int J Infect Dis 2006; 10: 43438.
in Japan, 20012006: emergence of high-level fluoroquinolone- 91 Dongol S, Thompson CN, Clare S, et al. The microbiological and
resistant strains. Epidemiol Infect 2010; 138: 31821. clinical characteristics of invasive salmonella in gallbladders from
67 Reed RP, Klugman KP. Neonatal typhoid fever. Pediatr Infect Dis J cholecystectomy patients in Kathmandu, Nepal. PLoS One 2012;
1994; 13: 77477. 7: e47342.
68 Muyembe-Tamfum JJ, Veyi J, Kaswa M, Lunguya O, Verhaegen J, 92 Chau TT, Campbell JI, Galindo CM, et al. Antimicrobial drug
Boelaert M. An outbreak of peritonitis caused by multidrug-resistant resistance of Salmonella enterica serovar Typhi in Asia and molecular
Salmonella Typhi in Kinshasa, Democratic Republic of Congo. mechanism of reduced susceptibility to the fluoroquinolones.
Travel Med Infect Dis 2009; 7: 4043. Antimicrob Agents Chemother 2007; 51: 431523.
www.thelancet.com Published online October 21, 2014 http://dx.doi.org/10.1016/S0140-6736(13)62708-7 9
Seminar
93 Chheng K, Carter MJ, Emary K, et al. A prospective study of the 114 Turner AK, Nair S, Wain J. The acquisition of full fluoroquinolone
causes of febrile illness requiring hospitalization in children in resistance in Salmonella Typhi by accumulation of point mutations in
Cambodia. PLoS One 2013; 8: e60634. the topoisomerase targets. J Antimicrob Chemother 2006; 58: 73340.
94 Commons RJ, McBryde E, Valcanis M, Powling J, Street A, Hogg G. 115 Accou-Demartin M1, Gaborieau V, Song Y, et al. Salmonella enterica
Twenty-six years of enteric fever in Australia: an epidemiological serotype Typhi with nonclassical quinolone resistance phenotype.
analysis of antibiotic resistance. Med J Aust 2012; 196: 33236. Emerg Infect Dis 2011; 17: 109194.
95 Kasper MR, Sokhal B, Blair PJ, Wierzba TF, Putnam SD. 116 Saha SK, Talukder SY, Islam M, Saha S. A highly ceftriaxone-resistant
Emergence of multidrug-resistant Salmonella enterica serovar Typhi Salmonella Typhi in Bangladesh. Pediatr Infect Dis J 1999; 18: 387.
with reduced susceptibility to fluoroquinolones in Cambodia. 117 AbdelGhani SM, Moland ES, Black JA, et al. First report of CTX-M-14
Diagn Microbiol Infect Dis 2010; 66: 20709. producing clinical isolates of Salmonella serovar Typhimurium from
96 Wu W, Wang H, Lu J, et al. Genetic diversity of Salmonella enteric Egypt. J Infect Dev Ctries 2009; 4: 5860.
serovar Typhi and Paratyphi in Shenzhen, China from 2002 118 Kumarasamy K, Krishnan P. Report of a Salmonella enterica serovar
through 2007. BMC Microbiol 2010; 10: 32. Typhi isolate from India producing CMY-2 AmpC -lactamase.
97 Phetsouvanh R, Phongmany S, Soukaloun D, et al. Causes of J Antimicrob Chemother 2012; 67: 77576.
community-acquired bacteremia and patterns of antimicrobial 119 Mushtaq MA. What after ciprofloxacin and ceftriaxone in treatment
resistance in Vientiane, Laos. Am J Trop Med Hyg 2006; 75: 97885. of Salmonella Typhi. Pak J Med Sci 2006; 22: 5154.
98 Nielsen MV, Sarpong N, Krumkamp R, et al. Incidence and 120 Morita M, Takai N, Terajima J, et al. Plasmid-mediated resistance to
characteristics of bacteremia among children in rural Ghana. cephalosporins in Salmonella enterica serovar Typhi.
PLoS One 2012; 7: e44063. Antimicrob Agents Chemother 2010; 54: 399192.
99 Keddy KH, Smith AM, Sooka A, Ismail H, Oliver S. Fluoroquinolone- 121 Diacon AH, Dawson R, von Groote-Bidlingmaier F, et al. 14-day
resistant typhoid, South Africa. Emerg Infect Dis 2010; 16: 87980. bactericidal activity of PA-824, bedaquiline, pyrazinamide, and
100 Frean J, Perovic O, Fensham V, et al. External quality assessment of moxifloxacin combinations: a randomised trial. Lancet 2012;
national public health laboratories in Africa, 20022009. 380: 98693.
Bull World Health Organ 2012; 90: 191199A. 122 Capoor MR, Nair D, Posti J, et al. Minimum inhibitory
101 Kariuki S, Revathi G, Kiiru J, et al. Typhoid in Kenya is associated concentration of carbapenems and tigecycline against Salmonella
with a dominant multidrug-resistant Salmonella enterica serovar spp. J Med Microbiol 2009; 58: 33741.
Typhi haplotype that is also widespread in Southeast Asia. 123 Kumar Y, Sharma A, Mani KR. Re-emergence of susceptibility to
J Clin Microbiol 2010; 48: 217176. conventionally used drugs among strains of Salmonella Typhi in
102 Smith AM, Govender N, Keddy KH, for the Group for Enteric, central west India. J Infect Dev Ctries 2011; 5: 22730.
Respiratory and Meningeal Disease Surveillance in South Africa 124 Engels EA, Lau J. Vaccines for preventing typhoid fever.
(GERMS-SA). Quinolone-resistant Salmonella Typhi in South Cochrane Database Syst Rev 2000; 2: CD001261.
Africa, 20032007. Epidemiol Infect 2010; 138: 8690. 125 Levine MM, Ferreccio C, Cryz S, Ortiz E. Comparison of
103 Neil KP, Sodha SV, Lukwago L, et al. A large outbreak of typhoid enteric-coated capsules and liquid formulation of Ty21a typhoid
fever associated with a high rate of intestinal perforation in vaccine in randomised controlled field trial. Lancet 1990; 336: 89194.
Kasese District, Uganda, 20082009. Clin Infect Dis 2012; 126 Wahdan MH, Sri C, Cerisier Y, Sallam S, Germanier R. A
54: 109199. controlled field trial of live Salmonella typhi strain Ty 21a oral vaccine
104 Mirza S, Kariuki S, Mamun KZ, Beeching NJ, Hart CA. Analysis of against typhoid: three-year results. J Infect Dis 1982; 145: 29295.
plasmid and chromosomal DNA of multidrug-resistant 127 Tacket CO, Ferreccio C, Robbins JB, et al. Safety and
Salmonella enterica serovar Typhi from Asia. J Clin Microbiol 2000; immunogenicity of two Salmonella typhi Vi capsular polysaccharide
38: 144952. vaccines. J Infect Dis 1986; 154: 34245.
105 Wain J, Kidgell C. The emergence of multidrug resistance to 128 Sur D, Ochiai RL, Bhattacharya SK, et al. A cluster-randomized
antimicrobial agents for the treatment of typhoid fever. eectiveness trial of Vi typhoid vaccine in India. N Engl J Med 2009;
Trans R Soc Trop Med Hyg 2004; 98: 42330. 361: 33544.
106 Al-Sanouri TM, Paglietti B, Haddadin A, et al. Emergence of 129 Martin LB. Vaccines for typhoid fever and other salmonelloses.
plasmid-mediated multidrug resistance in epidemic and Curr Opin Infect Dis 2012; 25: 48999.
non-epidemic strains of Salmonella enterica serotype Typhi from
130 Thiem VD, Lin FY, Canh G, et al. The Vi conjugate typhoid vaccine
Jordan. J Infect Dev Ctries 2008; 2: 295301.
is safe, elicits protective levels of IgG anti-Vi, and is compatible with
107 Phan MD, Kidgell C, Nair S, et al. Variation in Salmonella enterica routine infant vaccines. Clin Vaccine Immunol 2011; 18: 73035.
serovar Typhi IncHI1 plasmids during the global spread of resistant
131 van Damme P, Kafeja F, Anemona A, et al. Safety, immunogenicity
typhoid fever. Antimicrob Agents Chemother 2009; 53: 71627.
and dose ranging of a new Vi-CRM conjugate vaccine against
108 Holt KE, Phan MD, Baker S, et al. Emergence of a globally typhoid fever: randomized clinical testing in healthy adults.
dominant IncHI1 plasmid type associated with multiple drug PLoS One 2011; 6: e25398.
resistant typhoid. PLoS Negl Trop Dis 2011; 5: e1245.
132 Tran TH, Nguyen TD, Nguyen TT, et al. A randomised trial
109 Wain J, Diem Nga LT, Kidgell C, et al. Molecular analysis of incHI1 evaluating the safety and immunogenicity of the novel single oral
antimicrobial resistance plasmids from Salmonella serovar Typhi dose typhoid vaccine M01ZH09 in healthy Vietnamese children.
strains associated with typhoid fever. Antimicrob Agents Chemother PLoS One 2010; 5: e11778.
2003; 47: 273239.
133 Wang JY, Noriega FR, Galen JE, Barry E, Levine MM. Constitutive
110 Ahmed D, DCosta LT, Alam K, Nair GB, Hossain MA. expression of the Vi polysaccharide capsular antigen in attenuated
Multidrug-resistant Salmonella enterica serovar Typhi isolates with Salmonella enterica serovar Typhi oral vaccine strain CVD 909.
high-level resistance to ciprofloxacin in Dhaka, Bangladesh. Infect Immun 2000; 68: 464752.
Antimicrob Agents Chemother 2006; 50: 351617.
134 DeRoeck D, Ochiai RL, Yang J, Anh DD, Alag V, Clemens JD.
111 Capoor MR, Rawat D, Nair D, et al. In vitro activity of azithromycin, Typhoid vaccination: the Asian experience. Expert Rev Vaccines
newer quinolones and cephalosporins in ciprofloxacin-resistant 2008; 7: 54760.
Salmonella causing enteric fever. J Med Microbiol 2007; 56: 149094.
135 Karkey A, Thompson CN, Tran Vu Thieu N, et al. Dierential
112 Lee CJ, Su LH, Huang YC, Chiu CH. First isolation of epidemiology of Salmonella Typhi and Paratyphi A in Kathmandu,
ciprofloxacin-resistant Salmonella enterica serovar Typhi in Taiwan. Nepal: a matched case control investigation in a highly endemic
J Microbiol Immunol Infect 2013; 46: 46973. enteric fever setting. PLoS Negl Trop Dis 2013; 7: e2391.
113 Saha SK, Darmstadt GL, Baqui AH, et al. Molecular basis of resistance 136 Ochiai RL, Wang X, von Seidlein L, et al. Salmonella Paratyphi A
displayed by highly ciprofloxacin-resistant Salmonella enterica serovar rates, Asia. Emerg Infect Dis 2005; 11: 176466.
Typhi in Bangladesh. J Clin Microbiol 2006; 44: 381113.
10 www.thelancet.com Published online October 21, 2014 http://dx.doi.org/10.1016/S0140-6736(13)62708-7
You might also like
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Literarture ReviewDocument10 pagesLiterarture ReviewRiany Jade SabrinaNo ratings yet
- TNSS AU1.0 eng-USDocument1 pageTNSS AU1.0 eng-USRiany Jade SabrinaNo ratings yet
- Induction Labor Risks C-Section, PPHDocument16 pagesInduction Labor Risks C-Section, PPHRiany Jade SabrinaNo ratings yet
- TNSS AU1.0 eng-AUori ReviewDocument1 pageTNSS AU1.0 eng-AUori ReviewRiany Jade SabrinaNo ratings yet
- Ectopic Pregnancy: A Guide For PatientsDocument16 pagesEctopic Pregnancy: A Guide For PatientsRiany Jade SabrinaNo ratings yet
- Journal of Pediatric Surgery: SciencedirectDocument10 pagesJournal of Pediatric Surgery: SciencedirectRiany Jade SabrinaNo ratings yet
- Chapter IVDocument2 pagesChapter IVRiany Jade SabrinaNo ratings yet
- Occupational Skin Diseases in Construction Workers at A Large Construction SiteDocument3 pagesOccupational Skin Diseases in Construction Workers at A Large Construction SiteRiany Jade SabrinaNo ratings yet
- Allergic and Irritant Contact Dermatitis: Pathophysiology and Immunological DiagnosisDocument8 pagesAllergic and Irritant Contact Dermatitis: Pathophysiology and Immunological DiagnosisRiany Jade SabrinaNo ratings yet
- Chlamydia TrachomatisDocument12 pagesChlamydia TrachomatisEnrique S OcampoNo ratings yet
- Interventions For Hyperthyroidism Pre-Pregnancy and During Pregnancy (Review)Document12 pagesInterventions For Hyperthyroidism Pre-Pregnancy and During Pregnancy (Review)Riany Jade SabrinaNo ratings yet
- 1 Longitudinal Profiles of Thyroid Hormone Parameters in Pregnancy and Associations With Preterm BirthDocument15 pages1 Longitudinal Profiles of Thyroid Hormone Parameters in Pregnancy and Associations With Preterm BirthRiany Jade SabrinaNo ratings yet
- 1 Longitudinal Profiles of Thyroid Hormone Parameters in Pregnancy and Associations With Preterm BirthDocument15 pages1 Longitudinal Profiles of Thyroid Hormone Parameters in Pregnancy and Associations With Preterm BirthRiany Jade SabrinaNo ratings yet
- Accepted Manuscript: Respiratory MedicineDocument33 pagesAccepted Manuscript: Respiratory MedicineRiany Jade SabrinaNo ratings yet
- Current Chlamydia Trachomatis Infection, A Major Cause of InfertilityDocument7 pagesCurrent Chlamydia Trachomatis Infection, A Major Cause of InfertilityRiany Jade SabrinaNo ratings yet
- About My Needs?: Breadwinner, Provider or Pencari Nafkah'Document17 pagesAbout My Needs?: Breadwinner, Provider or Pencari Nafkah'Riany Jade SabrinaNo ratings yet
- Comparative Study in Infertile Couples With and Without Chlamydia Trachomatis Genital InfectionDocument9 pagesComparative Study in Infertile Couples With and Without Chlamydia Trachomatis Genital InfectionRiany Jade SabrinaNo ratings yet
- Chapter 4Document1 pageChapter 4Riany Jade SabrinaNo ratings yet
- Chlamydia Antibody Testing Helps in Identifying Females With Possible Tubal Factor InfertilityDocument6 pagesChlamydia Antibody Testing Helps in Identifying Females With Possible Tubal Factor InfertilityRiany Jade SabrinaNo ratings yet
- Surviving Sepsis Campaign 2016 Guidelines Presentation FinalDocument60 pagesSurviving Sepsis Campaign 2016 Guidelines Presentation FinalailedNo ratings yet
- 3116842klamidia Penyakit Menular SeksualDocument8 pages3116842klamidia Penyakit Menular SeksualRiany Jade SabrinaNo ratings yet
- Use of Epidural Clonidine For The Management of Analgesia in The Opioid Addicted Parturient On Buprenorphine Maintenance Therapy: An Observational StudyDocument6 pagesUse of Epidural Clonidine For The Management of Analgesia in The Opioid Addicted Parturient On Buprenorphine Maintenance Therapy: An Observational StudyRiany Jade SabrinaNo ratings yet
- Maternal Pulse Pressure and The Risk of Postepidural ComplicationsDocument11 pagesMaternal Pulse Pressure and The Risk of Postepidural ComplicationsRiany Jade SabrinaNo ratings yet
- Effects of Chlamydia Trachomatis Infection On Fertility A Case-Control StudyDocument7 pagesEffects of Chlamydia Trachomatis Infection On Fertility A Case-Control StudyRiany Jade SabrinaNo ratings yet
- Chapter 3Document1 pageChapter 3Riany Jade SabrinaNo ratings yet
- Abstrak CabeDocument1 pageAbstrak CabeRiany Jade SabrinaNo ratings yet
- 3Document8 pages3Riany Jade SabrinaNo ratings yet
- Table of ContentDocument1 pageTable of ContentRiany Jade SabrinaNo ratings yet
- Riany Jade IUGRDocument2 pagesRiany Jade IUGRRiany Jade SabrinaNo ratings yet
- 7 ReferenceDocument1 page7 ReferenceRiany Jade SabrinaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Fluid & Electrolytes Management (Nabil)Document78 pagesFluid & Electrolytes Management (Nabil)Ahmad Nabil Md RosliNo ratings yet
- Drug StudyDocument5 pagesDrug StudyMadsNo ratings yet
- Policies To Promote Child Health 25 Full JournalDocument204 pagesPolicies To Promote Child Health 25 Full JournalDiksha DuhanNo ratings yet
- Commonly Used Vet DrugsDocument31 pagesCommonly Used Vet DrugsIfran ChowdhuryNo ratings yet
- Non-Plaque Induced GingivitisDocument30 pagesNon-Plaque Induced GingivitisDentist AymanNo ratings yet
- Sportsdermatology: Skin Disease in AthletesDocument22 pagesSportsdermatology: Skin Disease in Athletesleticia floresNo ratings yet
- Pharma PPT TodocDocument40 pagesPharma PPT TodocPrincess Jovelyn GutierrezNo ratings yet
- Ii Anatomy+and+physiologyDocument2 pagesIi Anatomy+and+physiologybillyktoubattsNo ratings yet
- JSA - Doc Job Safety Analysis NewDocument3 pagesJSA - Doc Job Safety Analysis NewKali MuthuNo ratings yet
- Headache Chart PDFDocument3 pagesHeadache Chart PDFDavidVictoriousLukasNo ratings yet
- Local anesthetic bupivacaine nursing considerationsDocument2 pagesLocal anesthetic bupivacaine nursing considerationsPutuNo ratings yet
- Eva Madison QuestionsDocument2 pagesEva Madison QuestionsVictoria NarinesinghNo ratings yet
- Epidemiology - Exercises. Gaetano MarroneDocument4 pagesEpidemiology - Exercises. Gaetano Marronemillion assefaNo ratings yet
- Donatio Mortis CausaDocument6 pagesDonatio Mortis CausaJohn Phelan100% (2)
- Test Bank Chapter 6: Older Adults: Lewis: Medical-Surgical Nursing, 7 EditionDocument11 pagesTest Bank Chapter 6: Older Adults: Lewis: Medical-Surgical Nursing, 7 EditionBriseidaSolisNo ratings yet
- Mental Illness Annotated BibliographyDocument8 pagesMental Illness Annotated Bibliographyapi-386396722No ratings yet
- Journal of Anatomy - 2017 - Kirkpatrick - The Plantar Calcaneal Spur A Review of Anatomy Histology Etiology and KeyDocument9 pagesJournal of Anatomy - 2017 - Kirkpatrick - The Plantar Calcaneal Spur A Review of Anatomy Histology Etiology and KeyUlla NasNo ratings yet
- Argente v. West Coast Life InsuranceDocument2 pagesArgente v. West Coast Life InsuranceJellyn100% (1)
- 2006 Surgery Final 6th YearDocument13 pages2006 Surgery Final 6th Yearmarina_shawkyNo ratings yet
- Indoor Air PollutionDocument24 pagesIndoor Air PollutionMohamed SalemNo ratings yet
- Decompensated HFDocument16 pagesDecompensated HFJessica GarletsNo ratings yet
- The 25 Golden Rules of RunningDocument10 pagesThe 25 Golden Rules of RunningvivektonapiNo ratings yet
- PowerPoint DiabetesMellitusDocument175 pagesPowerPoint DiabetesMellitusDerlin NahariNo ratings yet
- IM Written Report Diabetes Case ReportDocument10 pagesIM Written Report Diabetes Case ReportJessa Mateum VallangcaNo ratings yet
- Glucose-6-Phosphate Dehydrogenase Deficiency - Overview: Symptom Treatment Prevention All InformationDocument2 pagesGlucose-6-Phosphate Dehydrogenase Deficiency - Overview: Symptom Treatment Prevention All InformationJinky TenezaNo ratings yet
- A Topic Presentation ON: Emerging Communicable DiseasesDocument52 pagesA Topic Presentation ON: Emerging Communicable DiseasesGiri SivaNo ratings yet
- Fine Tuning the Nutrition Care ProcessDocument13 pagesFine Tuning the Nutrition Care ProcessRacquel Jahn CorderoNo ratings yet
- Pelargonium SidoidesDocument2 pagesPelargonium SidoidesceramickurtNo ratings yet
- Mental Health Effects of ObesityDocument7 pagesMental Health Effects of ObesityMohd FaizNo ratings yet
- Tuberculosis in Pregnancy Effects Risks TreatmentDocument36 pagesTuberculosis in Pregnancy Effects Risks TreatmentOfel Santillan100% (1)