Professional Documents
Culture Documents
NFGSSSba WJW C
Uploaded by
Aryanto Dedy0%(1)0% found this document useful (1 vote)
9 views1,783 pagesnsw
Original Title
NFGSSSbaWjwC
Copyright
© © All Rights Reserved
Available Formats
PDF or read online from Scribd
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this Documentnsw
Copyright:
© All Rights Reserved
Available Formats
Download as PDF or read online from Scribd
0%(1)0% found this document useful (1 vote)
9 views1,783 pagesNFGSSSba WJW C
Uploaded by
Aryanto Dedynsw
Copyright:
© All Rights Reserved
Available Formats
Download as PDF or read online from Scribd
You are on page 1of 1783
Bonus
CD-ROM
Available!
See Back Cover
for More Details
The Science an
- Practice of Ph
21st EDITI
I,
is
24sT EDITION
Remington
The Science and Practice
of Pharmacy
(ium
WOAZ-F33-GD4 9
Editor: David B. Troy
‘Managing Editor, Matthew J. Hauber
Marketing Manager: Marisa A. O'Brien
Lippincott Williams & Wilkins
51 West Camden Stroot
Baltimore, Maryland 21201-2436 USA
530 Walnut Strost
Philadelphia, PA 19106
All rights reserved. This book is protected by copyright. No part ofthis book may be reproduced in any form or by any means,
including photocopying, or utilized by any information storage and retrieval system without written permission from the copy-
right owner.
‘The publisher is not responsible (as a matter of product liability, negligence or otherwise) for any injury resulting from any
‘material contained herein, This publication contains information relating to general principles of medical eare which should not
be construed as specific instructions for individual patients. Manufacturer's product information and package inserts should be
reviewed for current information, including contraindications, dosages and precautions.
Printed in the United States of America
Entered according to Act of Congress, in the year 1885 by Joseph P Remington, in the Office ofthe Librarian of Congress, at
Washington DC
Copyright 1889, 1894, 1905, 1907, 1917, by Joseph P Remington
Copyright 1926, 1936, by the Joseph P Remington Estate
Copyright 1948, 1951, by the Philadelphia College of Pharmacy and Science
Copyright 1956, 1960, 1965, 1970, 1975, 1980, 1985, 1990, 1995, by the Philadelphia College of Pharmacy and Science
Copyright 2000, 2006, by the University of the Sciences in Philadelphia
All Rights Reserved
Library of Congress Catalog Card Information is available
ISBN 0-7817-4673-6
‘The publishers have made every effort to trace the copyright holders for borrowed material. If they have inadvertently overlooked
‘any, they will be pleased to make the necessary arrangements at the first opportunity.
The use of structural formulas from USAN and the USP Dictionary of Drug Names is by permission of The USP Convention. The
Convention is not responsible for any inaccuracy contained herein.
Notice—This text in not intended to represent, nor shall it be intorproted to be, the equivalent ofor @ subslitute for the officiel
United States Pharmacopeia (USP) and/or the National Formulary (NB). In the event of any difference or discrepancy between the
‘current official USP or NF standards of strength, quality, purity, peckaging and labeling for drugs and representations of them
herein, the context and effect ofthe official compendia shall prevail.
‘To purchase additional copies of this book call our customer service department at (800) 638-8030 or fax orders to (301)
824-7390. International customers should call (901) 714-2824.
2845678910
Contents
1 Orientation
1 Scape of Pharmacy 3
2 Evolution of Pharmacy 7
3 thes and Protesienatism 20
4 ThePracice of Community Prarmacy 30
5 Phamacsts in Industry 35
5 Pharmacstsin Government 40
7 Pharmacsts and Public Heath 51
2 Infermation Resources in Pharmacy and the
Pharmaceutical Sciences 64
2 Circa orug tteraiure 74
10 Research 87
Part 2__ Pharmaceutics
11 Metrology and Pharmaceutical Calulations 99
Ta eT
13 Molecular Structure, Properties, and States of Matter ...162
14 Complex Formation 186
15 Thermodynamics 201
16 Solutions and Phase Equlibria. 20
17_Toné Solutions and Electrolytic Equilibria 231
18 Toniity, Osmoticty, Osmolaliy, ad Osmolanty 250
19 Chemica Kinetics 266
20 Interfacial Phenomena 280
21 Coloidaliepersions 293
22 Course Dispersions 319
23 Rheology 338
Part 3__ Pharmaceutical Chemistry
24 Inorganic Pharmaceutical Chemisty 361
25___Organic Pharmaceutical Cheristry 386
26 Naualmodes
27 Drug Nomendature—Unted States Adooted Names 443
28 Structure-Actty Relationship and Orug Design 468
29 Fundamentals of Nedica Radionucides 479
‘Analysis of Medcinals
495
Biological Testing 353
Clinical Analysis 565
Chromatography 599
Instumental Methods of Anaysis 633
35 Dissolution 672
Part Pharmaceutical Manufacturing
36 Separation 691
37 Powders 702
38 Property Based Drug Design and Preformulation . 720
39___ Solutions, Emulsiors, Suppensons, and Bxracts 745
40 Steilizaton 776
41° Parenteral Preparations 802
42 Intravenaus Admidures 37
43, Ophthalmic Preparations 250
44 Medicated Topicals a7
45 Oral Sold Dosage Forms 889
46 Costing of Pharmaceutical Desage Forms 928
47__Extendie-nelease and Targeted brug Delivery systems 939
48 TheNew Drug Approval Process ard
Clinical Trial Cesign 965
49. Biotechnology and Drugs 976
50 Aerosols 1000
St Quality Assurance and Control 1018
52___ Stability of Pharmaceutical Producte 1025
53 Bioavalabity and Bioequialency Testing 1037
5a Plast Packaging Materials 1047
Pharmaceutical 10
Part6 Pharmacokinetics and Pharmacodynamics
Diseases: Manifestations and P io 1085
57 Drug Abserption. Acion, and bispostion| Tad
58 Basic Pharmacokinetics and Pharmacodynamics 171
59 Cinial Pharmacokinetics and Pharmacodynames 1194
60 Principles of Immunology 1206
61 Adverse Drug Reactions and Clinical Toxicology 12
62 Pharmacogenomics 1230
63 Pharmacolinetic/Pharmacodyramics in
rug Development 1249
Part7__ Pharmaceutical and Medicinal Agents
64 Diagnostic Drugs and Reagents : 1261
65 Topical Orgs 1277
66 Gastointestinal and Liver Drugs 1294
67 Blood, Fluids, Electives, and Hematologcal rugs 1318.
68 Cardovascular rugs 1350
69 Respratory Drugs 1371
70 Sympathomimetic Drugs 1379,
71 Choinomimetic rugs 1389
72 Adrenergic Antagonsts and Ackenergic
Neuron Blocking Orugs ce 1399
73 Antimuscarnic and Antisposmodie O-ugs 1405
7a Skeletal Muscle Relaxants ant
75 Diuretic Dugs 1322
78 Uterine ard Animigraine Drugs 1432
77 Hormones and Hormone Antagonists 1437
78 General Anesthetics, 1474
79 Local Anesthetics 4479
80 Antiansety Agents and Hypnotic Drugs 1486,
81 Antiepileptc Drugs 1501
82 Paychopharmaclogie Agents 1509
83 Analgesic, Antipyretc, and Antrinfiammatory Drugs. ..1524
184 Histamine and Antinstamnic Drugs 1543
85 Centval Nervous System Simulants 1551
86 Antineoplastic Drugs 1556
87 _immunoactve rugs 1588
88 Parasticides 1595,
89 immunizing Agents and Allergen Extracts 1600
90 Antiinfecives 1526
91 Enzymes 1605
92 Nutrients and Associated Substances, 1688
93 Pestkides a9
Part® Pharmacy Practice
‘A. Fundamentals of Pharmacy Practice
94 ___ Application of Ethical Principles to Practice Dilemmas 1745
95 Technology and Automation 1753
‘36 “The Patient Rehavioal Determnanis 1762
‘97 Patient Communication 70
98 Patient Conplance 1782
99° Drug Education 1796
vod
2a
100
104
105
106
108
109
no
m2
na
14
16
‘CONTENTS
Professional Communications
‘The Prescription
Providing a Framework for Encuring
Medication Use Safety
Faison Contol
Drug Ineracions
txeemporaneous Prescription Compounding
‘Nuclear Pharmacy Practice
Nutrition in Pharmacy Practice
Pharmacoendemioiogy
Surgica Supplies
Health Accesories
B Social, Behavioral, Economic, and
‘Administrative Sciences
Laws Goverring Pharmacy
Re-engineering Pharmacy Practice
Prarmacosconomice
‘Community Pharmacy Economics and Managernent
Product Recalls ard Withdranals
‘Marketng Pharmaceutical Care Sevices
1808
1823
18a)
1881
1889
1903
1913
1925
1958
1968
1979
2015
2055
2070
2082
2098
2107
7
119
120
121
12
13
124
125
126
127
128
123
130
131
i
133
Documenting, Bling, and Reimbursement for
Pharmaceutical Care Senices
Pharmaceutical Risk Managerront
Integrated Health Care Delivery Sysiems
© Patient care
Specialization in Pharmacy Practice
Pharmacéts ard Disease State Management
Development ofa Pharmacy Care Pan and
Patent Problem-Solving
‘Amaulatory Patient Care
Self-Care
Diagnoste Set.care
Preventive Care
Hospital Pharmacy Practice
Emergency Medicine Pharmacy Practice
Long-Tern Care -
Aseptic Processing for Home Infusion Pharmaceuticals
Te Pharmacis's Role in Substance Use Disorders
Complementary and Alternative Metical Health Care
Chronic Wourd Care
aa
D24
2130
2155
2163
2170
2179
2197
2206
2223
2247
2265,
2272
2290
2303
218
2342
aa
You have either reached a page that is unavailable for viewing or reached your viewing limit for this
book.
aa
You have either reached a page that is unavailable for viewing or reached your viewing limit for this
book.
aa
You have either reached a page that is unavailable for viewing or reached your viewing limit for this
book.
PHARMACY PROFESSIONAL
DEGREE PROGRAMS
‘The following colleges and schools offering professional degree
programs in pharmacy hold membership in the ACP.
Alsbama Auburn University, Harrison Schocl of Pharmacy,
‘Aubur University, AL 36849
Samford University, MeWhorter Scheol of Pharmacy,
Birmingham, AL 35229
Arizona, Midwestern University, College of Pharmacy.
Glendale, Glendale, AZ 85808
University of Arizona, Colege of Pharmacy, Tueson,
AZ
Arkansos University of Arkansas for Medical Sciences, College
‘of Pharmacy, Lite Rec, ARR 72205,
California University of California, San Francisco, School of
Pharmacy, San Francisco, CA 94143,
University of the Pacific, Thomas J. Long School of
Pharemacy end Health Sciences, Stockton, CA 95211,
University of Scuthern California, School of Phar-
racy, Los Angeles, CA 90089
‘Western University of the Health Sciences, Collage of
Pharmacy, Pomona, CA 91766
Loma Linda University, School of Pharmacy, Loma
Tinda, CA #2350
University of California, San Diogo, School of Phar-
‘macy and Pharmaceatical Sciences, La Jolla, CA
2088
Colorado University of Colorado, Health Sciences Center,
School of Pharmacy, Denver, CO 8022
Connecticut University of Connecticut, Schoo! of Pharmacy, Storrs,
cr 0626s
Districtof Howard University, College of Pharmacy, Nursing
Cohimba and Allied Health Scieneor, Washington, LC 20089,
Flerida Florida Agricultural and Mechanical University, Col
luge of Pharmacy and Pharnaceatical Science, Talla.
hase, FL 32807
Nova Southeastern University, College of Pharmacy,
Fort Lauderdale, FL 33528
Palm Beach Atlantic Univesity, School of Pharmacy,
West Palm Beach, FL 33415
University of Florida, College of Pharmacy,
Gainesville, FL $2610
Georgia Mercer University, Southern Sehoo! of Pharmacy, At-
lanta, GA'30341
University of Georgia, College of Pharmacy, Athens,
GA.30502
Idaho Idaho State University, College of Pharmacy,
Pocatello, 1D 88208
Miinois Midwestern University, Chicago College of Pharmacy,
Downers Grove, IL 60515
University o Minos at Chicago, Collegeof Pharmacy,
Chicago, 1.60612
Indiana Butler University, Cellege of Pharmacy and Health
Purdue University School of Pharmacy and Pharma
‘eal Beionces, West Lafayette, IN47007
Towa Drake University, Cllege of Pharmacy and Health
‘Seencos, Des Mines, TA 60311
University oflowa, College of Pharmacy, lowa City, 1A
Kansas University of Kansas, School of Pharmacy, Lawrence,
‘0043
Kentucky University of Kentuehy, Collegeof Pharmacy, Lexing:
ten, 40536
Louisiana University of Louisiana at Monroe, Schoo! of Phar.
macy, Monme, LA 71209
Xavier University of Louisiana, College of Pharmacy,
‘New Orleans, LA 70125,
Maryland University of Maryland, Schoo! of Pharmacy. Balt
more, MD 21201
Massachusetts
Michigan
Minnesota
Mississppl
Missour
Montana
Nebraska
Nevada
Newdersey
New Mexico
New York
North Carolina
North Dakota,
Obie
Oklahoms
Oregon
Pennsylvania
Prerto Rico
(CHAPTER t: SCOPE OF PHARMACY 5
Massachusetts College of Pharmacy, and Health
Sciences Boston Campus, Boston, MA C2115
Massachusetts College of Pharmacy and Health
Scionces Worcester Campus, Worcester, MA 1610,
Northesstorn University, School o Pharmac, ston,
MAO2I05
Ferris State University, College of Pharmacy, Big
Rapid, MI 49807
University of Michigan, College of Pharmacy, Ane Ar
bor ME A808
Wayne State University, Bagone Applebaum Colege
of Pharmacy and Health Seienees, Detroit, MI 48202
Univernty of Minnesota, Calle of Pharmacy, Bie
neapols, MN 5
Univers of afassspp, School of Paarmaey, Uni
versity, MS 38655
St Louis Collegeof Pharmacy, St Louis, MO 63119
University of Missouri-Kansas City, School of Phar-
racy, Kanone Cis, MOBA110
University of Montana, School of Pharmacy and Aled
Health Science, Missoula, NT 59812,
Creighton Universit, School of Pharmacy nd Health
Prafessins, Omaka, NE 6817S
University of Nebraska Medien! Contor, College of
Pharmasy, Omaha, NE 68198
University ofSouthorn Nevada, Henderson, XV 89014
Rutgers, the State University of New Jersey, Ernest
Mario College of Pharmacy, Pieatatay, NU DB854
University of New Mexico, Collegeof Pharmacy, Alba
queue, NAESETSD
Union University, Albany College of Pharmacy, Al
tay, NY 1208
Long Island University, Armld and Marie Schwartz
College of Pharmacy and Health Sciences, Brooklyn,
NYT
St John's University, Cllege of Pharmacy and Aled
Heath Professions damaica, NY 11438
Site Univesity o'ew York at Bull, Shoal of Phar=
‘macy and Pharmaceutical Sciences, Amberst, NY 14260
Campbell University, Scheo! of Pharmacy, Buies
Creek, NC 27506
Univesity of North Carolina at Chape Hill, Schol of
Pharmacy, Chapel Hill. NC 27598
North Dakota State Universty, Callege of Pharmacy,
Fargo, ND 58108
Ohio Northern University, RAH. Raabe Collegy of
Pharmacy, Ade, O4 45810
‘The Ohio State University, College of Pharmacy,
Catumtan, OF 42210
University ofCincinnat, College a Pharmacy, Ciein-
tat OH 45957
University of Toledo, Cllegeof Pharmacy Tledo,OH
Southwestern Oklahoma State University, School of
Pharmasy, Weatherford, OR 709
University of Oklahoma, Callege of Pharmacy, Okla-
homa City, OK 75190
Oregon State University, College of Pharmacy, Cor-
vais, OR 97551
Dunuesne University, Mylan School of Pharmacy,
Pitsburgh, PA 15282
Lake Erie Clloge of Osteopathic Medicine, School of
Pharma. Ere, PA 16309
‘Temple University, Schl of Pharmacy, Philadelphia,
Paibna
University ofPituburgh, School of Pharmacy, Pat:
burgh, PA 15061
University ofthe Sciences in Philadephia, Philadel
‘hin Calloge of Pharmacy, Philadephie, PA 1910¢
Wilkes University, Nesbitt School of Pharmacy
Wikes-Barve PA L766
University af Puerto Ric, Scho! of Pharmacy, San
‘Jaan, PRON =
aa
You have either reached a page that is unavailable for viewing or reached your viewing limit for this
book.
aa
You have either reached a page that is unavailable for viewing or reached your viewing limit for this
book.
aa
You have either reached a page that is unavailable for viewing or reached your viewing limit for this
book.
essentially seperate, Cast to their own devices, monks put
together their own short versions of classical medical texts
(epitomes) and planted gardens to grow the medicinal herbs
that were no longer available after the collapse of trade and
commerce. Strong in their faith, these amateur healers tended
to ascribe their cures to the will of God, rather than to their
‘meager medieal resources.
‘As Western Europe struggled, a new civilization arose among.
those who fillowed the teachings of Mohammed (670-692), The
formerly nomadie peoples who united into the nations of Islam
conquered huge areas of he Middle East and Africa, eventually
expanding into Spain, Sicily, and Eastern Europe. Becausethei
fiath taught them to respect the written word and those whe
studied it, they tolerated the scholarship of the Christian sec
tarians whohad led persecution inthe Eastern Roman Empire,
the Nestorians, for example, established a famous school in
Gondeshapur in the 6th century.
‘Among the Islamic nations, Greek writings. including those
dealing with medicine, were translated into Arabic. At first the
‘Arabs accepted the authority of Greek medieal writings totaly,
‘especially those of Galen and Dioscorides. But as their sophis-
‘ication grew, Islamic medical men like Rhazes (860-032) and
Avicenna (980-1063) added to the writings of the Greeks. The
far-flung trading outposts ofthe conquering Arabs also brought
new drags and spices to the centers of learning. Moreover, Arab
physicians rejected the old idea shat foul-tasting medicines
‘worked best. Instead, they devoted a great deal of effort tomak-
ing their dosage forms elegan: and palatable, through the sil
‘vering and gilding of pills and the use of syrups.
“The new, more sophisticated medicines required elaborate
preparation. In the cosmopolitan city of Baghdad of the 9th cen-
fury, this work was taken over by specialists, the occupational
ancestors of today’s pharmacists. In places such as Spain and
southern Italy where the Islamic world interacted most with
Feeovering western Europe, several of the institutions and
developments of the more highly developed Arabic cultare—
such as the xeparation of pharmacy and medicine—pessed over
to the West.
‘By the mid.1th contury, when Frederick If, the ruler ofthe
Kingdom of the Two Sicilie, codified the separate practice of
pharmacy for the first ime in Europe, publie pharmacies had
ecome relatively common in southern Europe. Practitioners of
pharinacy had joined together within guilds, which sometimes
included dealers in similar goods, such as spicers or grocers, or
phiysicia
‘Arabic culture had returned classical scientific and medical
knowledge to Europe. At centers such as Toledo and Salerno,
the writings of the Grecks, which had been translated into,
Arabic centaries before on the fringes of the old eastern half
of the Roman Empire, were translated into Latin for the use of
European scholars. Thus, at the emerging universities of
Europe such as Paris(1150), Oxford (1167), and Salerno (1180),
scholars discussed the works of the great’ medieal authorities
such a Dioscorides, Galen, and Avicenna,
‘However, the debates on medicine among European aca-
omies wore based on speculation, not abservation. Theirs wat
‘a philosophical pursuit, with no great impact on medical prac-
tice, For significant change to occur in the use of druge, the
scholastic approach had to be set aside and a more skeptical,
observational methodology adopted. This new, experimental
lage we now call the Renaissance
THE RENAISSANCE AND EARLY
MODERN EUROPE
‘The Renaissance. simply put, was the beginning of the modern
period. Changes that had begun during the European Middle
Ager, and wore stimulated further by contacte with other
cultures, gained momentum. The burst of creative energy that
‘would result in our present shared culture ofthe West stemmed
not from a single episode, but from a series of events,
(CHAPTER 2: EVOLUTION OF PHARMACY 9
In 1453 Constantinople (Istanbul) fell to the conquering
‘Turks, and the remnants of the Greek schelarly community
there fled west, carrying their books and knowledge with them.
About that same time, Johann Gutenberg began printing,
‘with movable type, sterting an information revolution. Within
‘half century, Columbus discovered the New World, Vasco
da Gama found the rea route to Indie that Columbus had
sought, commerce based on money and banking was estab-
lished, and syphilis raged through Europe. [t was a time for
new ideas through reinterpretation of the old classical them
‘and through exploration on the high sea and in the laborator
‘The time was ripe for casting off the old concepts of diseases
‘and drugs of Galen. The new drugs that were arriving from far-
off lands were unknown to the ancients. Printers, after fulfilling,
the demand for religious books such as bibles’ and hymnals,
turned to producing medical and pharmaceutical works, espe-
cially those that could benefit from profuse and detailed illustra-
tions. On the medical side, for example, this trend is exemplified
in the anatomical masterworks of Andres Vesalius (1514-1564).
For pharmacy, printing had a profound effect on the study
of plant drugs, because illustrations of the plants could be re-
produced easily. Medical botanists such as Otto Brunfels
(1500-1534), Leonhart Fuchs (1501-1566), and John Gerard
(1545-1612) illustrated their works with realiatie renditions of |
plants, allowing readers to do serious field work or find the
‘Grugs needed for their practices, Among the most gifted of these
investigators was Valerius Cordus (1515-1548), who also wrote
‘a work ia another popular genee—formula books. His Dispen-
ssatorium (1516) became the official standard for the prepara-
tion of medicines in the city of Nuremberg and generally is
considered the first pharmacopeia.
Although they were critical to the advancement of medical
science, the nearly modern, precise works of Fucks and Vesal-
ius did not influence the treatment of disease as much as the
speculative, mystically tinged writings of an itinerant Swiss
surgeon who dubbed himself “Paracelsus.” Born Philippus
Aureolus Theophrastus Bombastus von Hohenheim in 1493,
the year Columbus went on his second trip, this medical
rebel represents well the combined attitudes of the common
man, the scholarly physician, the practical surgeon, and the
alchemist. The battles of Paracelsus against the static ideas of
Galen, Avicenna, and other traditional authorities opened a
window into the complicated mind of the Renaissance. As
Erwin Ackerknecht observed in A Short History of Medicine,
“Paracelsus is one of the most contradictory figures ofa contra
ictory age. He waa more modern than moet of his contempo
raries in his relentless and uncompromising drive for the new
and in his opposition to bind cbedience to aushoritariaaismand
books. On the other hand he was more medieval than most ofhis
contemporaries in his all;pervading mystic religiosity. His writ-
ings are a strange mixture of intelligent observation and mysti-
cal nonsense, ofhumble sincerity and boasting megalomania.”
Paracelsus was the most important advocate of chemically:
prepared drugs from crude plant and mineral substances, yet
he believed firmly that the collection of those substances
should be determined by astrology. He stated, again and
again, his total faith in observation while at the same time
preaching the “doctrine of signature,” a belief that God had
placed 2 sign on healing substances indicating their use
against disease (eg, liverwort resembles a liver, so it must be
{00d for liver ailments)
An outspoken enemy of university-edueated physicians,
Paracelsus denigrated their scholasticism and wrote his own
works in his native language rather than in the traditional
Latin. He harshly criticized pharmacy practitioners as vell,
even though his advocacy of chemically prepared medicin«
was to spark the growth of the modern pharmaceutical sci-
fences. Chemical processes, especially distillation, empowered
the follower of Paracelsus to isolate the healing principles of a
drug, ite quintessence. Eventually, as the efficacy of some of
these drags became known, they entered professional medical
aa
You have either reached a page that is unavailable for viewing or reached your viewing limit for this
book.
aa
You have either reached a page that is unavailable for viewing or reached your viewing limit for this
book.
aa
You have either reached a page that is unavailable for viewing or reached your viewing limit for this
book.
immigrants from the Continent, where states often restricted
pharmaceutical practice, expressed opposition to the legal
Control of pharmacies. Many had come to North Ameriea to
fpen their ovn shops, rather than wait years in their native
lands for permission.
nthe late 1860s the academie model of professionalism be-
ing worked out by other so-called "new professions” such ax
engineering attracted the attention of some pharmaceutical
leaders. Using university degrees, plus state licensing or in-
stitutional certification, these new professions set themselves
apart fom other occupations as “communities of the compe-
tent.” They sought to avoid the ordeals of the marketplace by
putting a cognitive gap between their work and the publics
Understanding. Theoretically, by controlling admissions to
professional schools and raising examination standards, de-
structive competition could he reduced or even eliminated
LEGISLATION
‘The APhA responded to the movement ofthe late 1860s toward
increased public protection and occupational security through
law by publishing a model pharmacy act. Physicians and others
concerned with the safe use of poisons and potent drugs had
petitioned state legislatures for laws governing pharmacy. Ini-
tally, pharmacists took @ negative view, reacting to the idea
that physicians or bureauerats would gain authority over phar-
macy practice via state inspectors or licensing beards. To
‘ensue that the profession's best interests would be protected,
the APhA empowered a committee to draw up a model law.
Refecting the ambivalent attitude of many pharmacists to.
ward legal regulation, the APhA published and distributed
their model law without endorsement. As small businessmen,
pharmacists did not want outside restriction on their trade.
During the 1870s state legislatures began considering
ceamest pharmacy bills sponsored by nonpharmacists. Reacting
to this trend, pharmacists organized statewide associations to
coordinate support for their own bills, which were often ver-
sions of the APhA model. Although not enthusiastic at first
about regulation of their businesses, pharmacists wanted @
voice in the process. The eventual success oftheir efforts in the
1870s, 1880s, and 1890s evinced a changing attitude toward
the pursuit of professionalism from the 186(s.
‘The bourdary hetween masters of the pharmaceatical art
and mere store clerks, which had always been flimsy, was dix
intograting Pharmacists sought new ways to demonstrate their
competence and to separate themselves from ignorant drug sell
cersand quacks. The evidence for this expertise, however, shifted
away from individual achievement in the marketplace toward
group identification and institutional certification.
TRANSITION TO A MODERN PROFESSION
‘The period between 1870 and 1920 was transitional for both
pharmacy and pharmaceutical education. Before the Civil Wat
perhaps only 1in20 American pharmacists had finished formal
Schooling in pharmacy, which had consisted of night courses to
supplement apprenticeship training. With the passage of state
Jaws requiring the examination ane registration of pharmacists
from the 1870s on, pharmacy became part of the wave of pro-
fessionalization sweeping across American society. The new
professionals based ther claims of status on their diploma and
licenses, not their preducts
Pharmacy got caught up inthis trend, and evea though state
laws did not require a pharmacy schoo diploma for Heensure
‘until the early 20th eentury, the prestige attached tothe sheep-
skin attracted students tothe burgeoning numberof school, as
public expectations inereased and “professional” became ®
coveted ttle
Pharmaccutical education around the turn of the century
was related closely to practice as pharmacisteducators such as
‘Joseph Remington replaced the physicians and other nonphar
‘CHAPTER: EVOLUTION OF PHARMACY 13
macy practitioners who had dominated the earlier schonls. Stu-
dents also had a wide range of possible educational experiences.
+ Short-term cram schools were available for these who just wanted
to pase a state board exam.
+ Small, loal schools sprang up in medium size cities offering basic
instruct and large diplomas for display.
+ The old-lin schools, affibated with loea! pharmaceutics! organi-
zations, provided students with excellent practical edueation, plus
fan opportunity to explore specialty areas, depending on te cl
lege faculty.
+ Starting with the University of Michigan in 1858, sehools of
pharmacy alibated themselves with state colleges and univers-
‘ies; a trend that altered the direction of American pharmacet
cal education
As part of larger university communities, these pharmacy
schools aspired to the high standards of scholarship exhibited
by established disciplines and other professions. The leaders of
the university faculties helped transform pharmaceutical edu-
cation from a vocational to a scientific orientation through
Pharmacy programs that emphasized fulltime coursework and
laboratory study.
‘During this period pharmacy’s part in health care salidified,
the dispensing of medicines by physicians deslined. How.
ever, the rise of the cut-rate drugstore and, more importantly,
the chain drugstore, also oowurred during these 50 year, which
further increased economic pressure on the profession.
Bill, most pharmacists worked in their wn corner drug
store, which became a fixture in American life withits shelves of
patent medicines forall ils and a seda fountain for delighiful
beverages; the proprieior, often called doc, atiended to the mi-
nor aches and pains of customers or made chocolate sodas with
equal skill Although the pharmacist relied on prescription com
pounding for his professional identity, this provided only a small
Fraction ofhis income. To proteet this independent and uniquely
‘American style of practice from the incursion oflarger retailers,
the National Association of Retail Draggists (NARD) w:
founded in 1898. At first the APhA weleomed and cocperat
with he new aational organization, but the spit that eventually
developed between the APhA, which was oriented to scientific
and professional advancement, and NARD, which concentrated
on the individual commercial success of owners, weakened the
profession's voice in national affairs in the years to come.
was an exciting time in medicine, with therapeutics un-
dergoing a transformation. The germ theory of disease, cham
pioned by laboratory scientists such as Louis Pasteur and
Robert Koch, resulted in significant immunotogical advances in
the 1880s and 1890s. Pasieur's rabies vaccine and Frail von
Behring’s diphtheria antitoxin demonstrated that cures for
infectious disoases could arise from the laboratory. Paul
Ehriich transcended the biological effors of his predecessors
when he introduced Salvarsan in 1910, the first chemothera-
peutic agent. Although it fll short of Ehrich’
bullet, which could destroy microorg
damaging the patient, Salvarsan did inspire others ta search
for drugs with chemotherapeutic potential. Aside fom the
biologicals, however, few ofthe drugs discovered during the late
19th and early 20th centuries had significant impact on the
prevention or cure of disease.
Industral research on érugs produced several new agents,
such as the analgesic and antipyretic aspirin or the sedative
chloral hydrate, that reduced the pain and sulfering associated
With illness. Even though pharmacior sorved as important
Outlets for sera, antitorins, and vaccines, mos ofthe medicines
compounded or sold by pharmaciats around the turn of the
century eased symptoms, rather than treated roa illnesses.
'As scientific pharmacolegy explained how drugs werked on
a cellularandorgan system level, the concept of drags and their
Actions held by professionals and laypeople diverged. The pub-
lic clung to outdated ideas of humoralism augmented by a
rmodicum of germ theory. Such beliefs made eonsumers suscep-
tible to patent medicine advertising, which misled them into
equating the effets of strong laxatives and analgesics with the
aa
You have either reached a page that is unavailable for viewing or reached your viewing limit for this
book.
aa
You have either reached a page that is unavailable for viewing or reached your viewing limit for this
book.
aa
You have either reached a page that is unavailable for viewing or reached your viewing limit for this
book.
Medisinalordnung Friedrichs II. Rine phormatiehistorische
Studie (Eutin: Internationale Gesellschaft far Geschichte der
Pharmazio, 1957). In he poriodicaliterature, not particularly
the writings of Alfons Lutz, euch as “Der verschollene frih-
salernitanische Antidotarius magnus - "and itsrich bibliogra-
phy (new series, vol 16; Stuttgart: Veroffentlichungen der
Internationalen Gesellschaft fur Geschichte der Pharmazie,
1960, pp 97-183}; also see the works of Rudolf Schmitr, such
+... Apothekerstandes im Hoch und Spat-Mittelalter” (val 18;
Stuttgart: Verofentlchungen der Internaticnalen Gesellschaft
fur Geschichte der Pharmazie, 1958, pp 187-165) ard “Ueber
deutsche mittelateriche Quellen zur Geschiehte von Pha
marie und Medizin” (Deut Apotheker-Zig 1960; 100: 980). En-
lish language studion of snunoal value and clarity include
articlesby GE Trease, such as “The Spicers and Apothecaries of
the Royal Household in the Reigns of Henry Il, Bdward I and
Edward" (Nottingham Mediaeval Studiesi969;3: 19;abridged
in Pharm J,4 April 1949, pp 246-248). A uniquely useful work
is Sister Mary Francis Xavier [Welhoefer], Statutes ofthe Guild
of Physicians, Apothecaries and Merchants in Florence
(1313-1816, A Brief Commentary, with ar Introduction and
‘Transletion,” (unpublished PhD dissertation, University of
Wisconsin, 1988), even though itis dated as to many details. On
metieval European materia media, see Henry E Sigerist, Ma-
teria Madica in the Middle Ages” (Bull Hist Med 1998; 7: 417),
and his“Studien und Texte zur frikmittelalterlichen Rezeptlt:
ratur” (ol 13; Leipzig: Studion zur Gosehichte der Medizin,
1923, pp 187M. Probebly the eerliest pharmacists texibook and
‘mantal hasbeen translated into German by Leo Zimmermann,
Saladini de Aseulo.... Camperdium aromatariorum (Leipzig,
1919); for « Hebrew translation, see Suessmann Muntner,
editor, Sefer ha-rokhim (Tel-Aviv: np, 1953).
‘On Modern Europe: For a reliable and concise medical
overview, seo Erwin Ackerknecht, A Short History of Medicine
(New York: Ronald Press, 1958); for detailed references, supple:
‘ment itwith Fielding Garrison, An Introduction to the History
of Medicine, 4th ed Philadelphie: Londen: WB Saunders, 1929;
‘epublished 1960), noting ospaialy the bibliographic oxaays of
‘Appendix IL. Some international survey volumes on pharmacy,
with particular reforence to the modem period, ae listed in
Sonnedecker and Berman's Sone Bibliographic Aids for Histor
ical Writers in Pharmacy (Madison, WE American Institute of
the History of Pharmacy, 1958). A gap has been closed, mean
while, by Leslie G Matthews, History of Pharmacy in Britain
(Edinburgh and London: E & S Livingstone, 1962) and Cecil
Wall, HC Cameron, and EA Underwood, A History of the Wor-
shioful Society of Apothecaries of London, VolT: 1617-1815 (Lon-
don: Oxford University Press, 1963). For those contemplating
research in British archives, se [-Richmond, J Stevenson & A
‘Turton, eds, The Pharmaceutical Industry: A Guide to Histor
cal Records (Buslington, VT: Ashgate, 2003) There is not yet 4
comprehensive, up-to-date history tha: deals with Buropean
pharmacy; ibllographies, such aa those cited in the earlier sec
tion on general literature guides, will yielé books and mono-
graphs from particular topleal and national viewpoinis. For an
example of e specialized topic, see Richard Palmer, ‘Pharmacy
in the Republic of Venice," in The Medical Renaissance ef the
Siateenth Century, A Weer, editor (New York: Cambridge Uni-
versity Press, 1985); see aloo B Potesch editor, The Pharmacy
Windows on History (Rocke, 1996). specialized book of note
M.S. Conroy, In Health and Sickness: Pharmacy, Phormacist
and the Pharmaceutical Industry in Late Imperial, Early Soviet
‘Russia (New York, Columbia University Press, 1984). Espe-
cially rich ip Europoan history are the publications, 1927 tothe
present, of the International Society for the History of Phar
macy; « partial key has been published by Herbert ftugel, Die
“Veroffentlichungen der Internationalen Geselischaf fur
Geschichte der Pharmazie 1955-1965: Eine Bibliographic" (new
series Bd 29; Stuttgart: Veroffentichungen der Internationalen
Gesellschaft fur Geschichte der Pharmazie, 1967).
‘On the US: The standard volume in English, Kremers and
Undang's History of Pharmacy, revised by Glenn Sonnedecker
CCHAPTER2: EVOLUTION OF PHARMACY 17,
(Philadelphia: Lippinestt, 1976), devotes approximately two-
thirds ofthe main text to the United States, and its bibliogra-
phies open up a wide range of other American literature. Note-
‘worthy are the anniversary issues of Druggists Cireular vol,
Tanuary 1007 and Pharmaceutical Era vol 16, no 27, 91 De”
‘comber’ 1896). Seo also Glenn Sonnedecker, “Structare and
Stress ofAmerican Pharmacy" (Pharm J, 14 April 1996, pp 3-8)
A series of 18 historical articles on American pharmacy were
published in J APiA during 2000, 2001, and 2002. Four papers
covering a wide variety of American topies are contained in GJ
Higby & BC Stroud, eds., Apothecories and the Drug Trade
(Madison: American Insti ofthe History of Pharmacy. 2001)
‘The story of American pharmacy’s umbrella organization is told
by Goonge Grifonhagen, 150 Years of Caring! A Pictorial Hix-
tory ofthe American Pharmaceutical Association (Washington,
DC: APhA, 2002). Pharmaceutical education is explored in
depth by Robert A. Buerki, “In Search of Excellence: The First
Century ofthe Ameriean Assoriation of Colleges of Pharmacy,”
‘Am Pharm Ea 63 (Fall Supplement 1999) 1-210. A useful bok
at certain aspects of colonial American pharmacy can be found
in Renats Wilson, Pious Traders in Medicine: a German Phar-
rmaceutical Network in ighteenth-Century North America (Uni-
versity Park, PA: Pennsylvania State University Press, 2000)
Several different aspects of 1thcentary practice are considered
by Gregory Highy, In Service to American Pharmacy: The Pro-
fessional Life of William Procter, Jr Tuscaloosa: University of
Alabama Press, 1902). A solid Biography of @ 20th-contury
‘American pharmacist is James Madison, Elf Lilly: A Life,
1685-1977" ndianapslis: Indiana Historical Society, 1989)
Other valuable biographies include Michael A Flannery, John
Uri Loyd: The Great American Eclectic (Cartondale: Southern
Mlinois University Press, 1998) and Sabine Knoll-Schiize,
Friedrich Hoffmann (1832-1904) ond the ‘Pharmaccutische
Rundschau’ (New York: Peter Lang, 2008). Changes in the use
and production of drugs are explored by John Harley Warner,
‘The Therapeutic Perapective: Medical Proctce, Knowledge, and
Identity in Americ, 1820-1885(Cambridge: Harvard Univer-
sity Prose, 186) and John P Swann, Academie Scientists and
the Phermaceutical Industry: Cooperative Research in
‘Twentieth: Century America Baltimore: ohne Hopkins Univer-
sity Press, 1988). See also John Parascandola, The Development
of American Pharmacology: John J. Abel and the Shaping of a
Discipline (Baltimore: Johns Hopkins University Press, 1992)
and Harry M Marks, The Progress of Experiment; Science and
Therapeutic Reform in the United States, 1900-1990 (Cam-
bridge, UK; New York: Cambridge University Press, 1997).
Short histories of individual drugs are provided by Walter
Sneader, Drug Prototypes and Their Exploitation (New York:
‘ohn Wiley, 19961 For a contemporary ase of historieal argu
‘ments in poly analysis, se a series of articles written by RW.
Holland & CM Nimmo on “Transitions in Pharmacy Practice,”
that appear in the Amer J Health-System Pharm 56 (1999):
1758-64, 1981-7, 2254-41, 2458-62, 67 (2000) 64-72. A usoful
bibliography that is stil in prints by George Griffenhagen, Bib
ography of Papers Published by the American Pharmaceutical
‘Associaton that were presented before the Association's Section
‘on Historical Pharmacy, 1904-1967 (Madison, WI: American In-
stitute ofthe History of Pharmacy, nd), which includes subject
and author indexes; although it emphasizes American history,
it isby no means restricted to it The “Pharmacy” section ofthe
annual bibliography inthe Bulletin of the History of Medicine at
‘one time offered an important key ta the literature, which wax
cumulated in Bibliography of the History of Medicine of the
United States and Canada, 1989-1960, Genovieve Miller, editor
‘Baltimore: Johns Hopkins University Press, 1964). See also
other bibliographies listed earlier in the section on general li
erature guides. Also noteworthy is the “Bookshelf” section of
Pharmagy in History, « quarterly ofthe American Institute of
the History of Pharmacy (Madison, WI); and the sections on
“History and Ethics," “Sociology and Eeonomie,” and “Litera-
ture" in the ongoing International Pharmaceutical Abstracts
(Washington, DC: American Society of Hospital Pharmacist)
aa
You have either reached a page that is unavailable for viewing or reached your viewing limit for this
book.
aa
You have either reached a page that is unavailable for viewing or reached your viewing limit for this
book.
aa
You have either reached a page that is unavailable for viewing or reached your viewing limit for this
book.
Preamble
Pharmacists are health professionals who assist individu-
alsin making the bes: use of medications. This Code, pre-
pared and supported by pharmacists, is intended to state
publicly the principles that form Uefundamental basisof the
roles and responsibilities of pharmacists. ‘These prin-
ciples, based on moral obligations and virtues, are estab-
Ushed to guide pharmacists in relationships with patents,
professionals, and society.
1. A pharmacist reapecta the covenantal relationship be-
tween the patient and pharmacist.
Considering te paten-phamacit rations asa covenant means
that maral obligations in response to the gift of trust
freshedivom socey. nretan forts git pharmacist promises
help individuas achieve optimum benefit rom their medications, to be
‘Corti to thelr welfare ancora el trast
IL. A pharmacist promotes the good of every patient ina
caring, compassionate, and confidential manner.
{A pharmacist places concern forthe wel-beg ofthe patient atthe
ceruer of professional practice. In doing s0, a pharmacst considers
‘eed tase by the pation’ arwellas howe definedby heatracience. A
[Pharmacist is dedicated to protecting the dignity ofthe patent. With
faring atte and s compassionate spits pharmack focus on
‘serving ke patent na private and confidential anne.
TIL A pharmacist respects the autonomy and dignity of
each patient.
promotes the right ose determination and recognizes
indvidon eros by ecouri patent partiae in decisions
about thar health A pharmacist communicates wit patients interns
that are understandable. In all cases a pharmacist respects persoral
and cultural diferences among patents
Code of Ethics
American Pharmacists Association
CHAPTER 2: ETHICS AND PROFESSONAUSM 21
IV. A pharmacist acts with honesty and integrity in profes-
sional relationships.
‘A pharmacist ha aduty otllthe truth and to act wih conviction of |
constience. A pharmacist avoids tory practices, behavior o |
‘work conditions that impr professional Jaden, snd artlons that
Compromise deacation wo ve bes iverests of paris
V. A pharmacist matnains professional competence.
A pharmacist has a duty to maintain knowledge and ables as new
‘medieators, devices, and teehndlogies became available and as fealth
Information advances
VI._A pharmacist respects the values and abilities of col-
leagues and other health professionals.
‘When appropriate, a pharmacletanks forthe consultation of cot
leagues or other health professcnas or refers the patient. A pharma-
at kn ‘that colleagues and other heath professionals may
ifferin the belles and values they appy tothe cae ofthe patient.
VII. A pharmacist serves individual, community, and soci-
etal needs,
‘The prinary obligation of a pharmacist i to individual patents.
However, the obligations oa ptarmacit tay at snes extend yon
the Individual to the community and society. Ie these situations, the
Dpharmaclat cognac: the raponsiiltics tt actompany these osiga
onsand acts accordingly.
VII. A pharmacist seeks justice in the distribution of health
‘Wen health resources are located, a pharmacist i fair and equ
cable balareing te needs of patents ad sore.
Figure 3-1. Code of ethic (Originally published in “Code of Ethics for Phamacis.” Am J Healt-Syst Pham 1995: 52: 2131. © 1995, American
Society of Health-System Pharmacists, Inc All ights reserved. Reprrted with permission.)
‘The second characteristic of a professional is 2 set of specific
‘attitudes that influence professional behavior. The basic com-
ponent of this set of ettitudes is altruism, an unselfish concern
for the welfare of others:
“The professional man, it has been said, does not work in order
to be paid: he is paid in order that he may work. Every decision
hhe makesin the course f his career is basedon his sense of what
is right, not on his estimate of what is proftable”*
Professionals are concerned with matters that are vital to the
‘health or well-being of their clients, The practitioner employs
highly specialized technical knowledge, which the patient or
client does not possess. Both the client's lack of knowledge and
the vital nature of professional services provide the profes-
sional with an opportunity to exploit the client. The conse-
‘quences of such exploitation are severe. The smocth functioning
of the professions requires that the practitioner must consider
the needs of the patient as paramount, relegating his or her
‘own material needs to an inferior posito
Social sanction, the third characteristic of a professional, i
a resultant effect of the two characteristics already discussed.
Whether an occupation is considered to be a profession de-
pends, to a large degree, on whether society views it as such.
One measure of social sanction is the granting of exclusive
rights of practice through the licensing power of the state,
Licensing not only attempts to protect the public from in-
competent practitioners, but also frequently creates a relation-
ship of trust between society and the professionals, because
‘within the sphere of professional activities, the professional ex-
ercises an authoritative power over pationts. As explained by
Greenwood,
“(he professional dictates what is good or evil for the client,
‘who has no choice but to accede to professional judgment. Here
the premise is that, because he [or she] lacks the requisite theo-
ratieal background, the elient eannot diagnose his [or hor] own
‘needs or discriminate among the range of possibilities for meet-
ing them."
‘Theextent of the public's trust is a measure of the degree of so-
ial sanction, and this is evident in society's permitting the ex-
cercise of sovereign power over professional matters. Given the
‘egal monopoly inherent in professional licensing, the failure of
society ta impose further centrale on the profession is sanction.
ing, by implication, the profession's performance and selfregu-
lation. Thus, profeaeions have evolved as occupations connected
with high status. The functional relationship of professions to
aa
You have either reached a page that is unavailable for viewing or reached your viewing limit for this
book.
aa
You have either reached a page that is unavailable for viewing or reached your viewing limit for this
book.
aa
You have either reached a page that is unavailable for viewing or reached your viewing limit for this
book.
grants approval for its release. Confidentiality and privacy
have received a great deal of attention recently with the pas
\ge and implementation of the Health Insurance Portability
and Accountability (HIPAA) Act.
‘Though often used interchangeably, the terms confidential
ity and privacy do differ. A violation of privacy occurs in situa-
tions where personal information is obtsined/revealed by an in-
dividual who has not been granted access to such information,
A compater hacker would be an example, Conversely, a viola
tion of confidentiality results from the inappropriate release of
personal information to others by a person, such as a health
care professional, who has been granted access to such
information
Tn healthcare, it ix somotimes unclear which members of the
health care team may have access to confidential medical
records without the express consent of the patient, Should
pharmacist or physical therapist earing for a patient have the
same access to medical records that is afforded the patient's
physician or hospital nurse? Another difficult ethical situation
wolves a patient who explicitly expresses a desire not to have
formation divulged to a member of the health care team. For
example, a patient may tell a pharmacist of her decision to al-
ter her prescribed therapeutic regimen, but request that the
pharmecist not disclose this information to her physician.
Confidentiality has the same two ethically justifiable ex-
ceptions as does the principle of sutonomy, the harm princ-
ple, and weak paternalism. As with autonomy, a pharmacist
‘may be ethically justified in violating the confidentiality of @
patient when keeping information private may harm others
(harm prineple) or when the patient lacks autonomy (weak
paternelism)
Beneficence/Nonmaleficence
Ronoficence and nonmaleficence are ethical principles that are,
in a sense, complimentary to one another. Beneficence indi
cates that you act in a manner to do good. Nonmaleficence
refers to taking due care or avoiding harm. Beauchamp and
Childress compare these related principles
‘The word nonmaleficence is sometimes used more broadly to
inelude the prevention of harm and the removal of harmful con-
ditions. However, because prevention and removal require pos-
itive acts to assist others, we include them under beneficence
along with the provision of benefit. Nonmaleticence is restricted
to the noninflietien of harm.
Fidelity
Fidelity requires that pharmacists act in such a way as to
demonstrate loyalty to their patients. A type of bond or promise
is established between the practitioner and the patient. This
professional relationship places on the pharmacist the burden
of acting in the best interest of the patient, Pharmacists have
an obligation of fidelity to all their patients, regardless of the
length of the professional relationship. In community phar-
macy, for example, practitioners have the same obligation to
show fidelity to an oceasional patient as they have for a regular
vastomer
‘The depth of the fidelity relationship between the pharma-
cist and patient is a topic of ongoing discussion among phar.
‘macy ethicists, Two forms of fidelity are frequently alluded to:
covenantal and contractual, Covenanial fdelity is often de-
scribed as an intimate and spiritual commitment between indi
viduals. Examples would inclade the fidelity of marriage and
the fidelity between a member ofthe elergy and his or her con-
gregation, Conversely, contractual fidelity does not involve &
level of commitment beyond that owed another as the result of
a binding agreement. An example of this form of fidelity would
be the relationship one might have with a eontractor such as a
plumber or electrician. What remains in dispute is where the
(CHAPTER: ETHICS ANO PROFESSIONALISM 25,
pharmacist-patient relationship lies along the continuum be-
tween covenant and contract
Verscity.
bbe honest in their dealings with patients. There may be times
when the violation of veracity may be ethically justifiable (as
with the use of placebos), but the violation of this principle for
‘non-patient-centered reasons would appear to be unethical. In
1 professional relationship based upon professional fidelity, pa-
spect that their pharmacist will be
Distributive Justice
ibutive justice refers to the equal distribution of the bene-
fits and burdans of society among all members of this socioty.
We often think of distributive justicein terms of our health care
delivery system. This principle is frequently used as a jastfica-
tion for providing health care as a right to all Americans.
Even though justice instructs that pharmacistsdemonstrate
an equivalent amount of care, pharmacists do not always pro-
vide care with equal fervor to all patients. Sadly, issues such as
the patient’ socioeconomic status often impact the level andi
tensity of eare provided by health care professionals. Medicaid
patients are sometimes provided a much lower quality of care
than a patient who is a cash-paying customer or who has a full-
coverage drug benefits plan. All too often, the eare provided by
a health care professional is viewed in terms ofthe personal re-
‘ward for the professional, euch ax the level of reimbursement
the care is likely to reap. Justice demands that the focus be on
patients and theirmedical needs, not on the financial impact on
the health eare professional."
ETHICAL CODES
Ethical principles and rules that apply to medical practice and.
research, such as autonomy, beneficence, and justice, have long
served as the basis for a system or code of ethical conduct.
‘Western medical ethics is primarily based on the Hippocratic
code attributed to the Greek philosopher Hippocrates, 5th cen-
‘tury RC Medicine (American Medical Association) and phar-
macy (Philadelphia College of Pharmacy) developed codes of
conduct for their respective practitioners in 1848. As Montagne
notes, “the guiding principles of these eodes were a respect for
human life aad service to humanity.” The Holecaust during
World War Il, and the subsequent Nuremberg trials, would
prompt the first major development of a code dealing speci
cally with experimentation on human subjects.
‘Subsequent to Nuremberg, several other codes of medical
ethics were established. In 1949, the World Medical Association
drafted the Geneva Convention Code of Medical Ethics, a eon-
temporary version of the Hippocratic oath. In the 1960s, the
‘same organization established an ethical code on clinical re-
search. In 1984, the Declaration of Helsinki was adopted based
‘upon the Nuremberg principles, and it was further revised in
1975. In 1972, the American Hospital Association issued a
Statement ona Patient's Bill of Rights. In 1977, the Declaration
of Hawaii provided ethical guidelines for clinical research in
psychiatry.
‘Ethical cotes provide health care professionals with ethical
principles and standards by which to guide their practice, How-
ever, ethical principles and codes cannot hope to provide health
care professionals with answers to every moral question that
‘may arise in the course of their practice. Ethical questions in
health care involve decision-making that is usually situation-
specific. The purpose of such principles and codes is not to pro-
vide practitioners with right and wrong answers, but to offer
them a framework to use when faced with ethical questions. As
You might also like
- AbstractsDocument1 pageAbstractsAryanto DedyNo ratings yet
- 26Document13 pages26Aryanto DedyNo ratings yet
- 26Document13 pages26Aryanto DedyNo ratings yet
- Evaluasi Keamanan DendiMoyDocument9 pagesEvaluasi Keamanan DendiMoyAryanto DedyNo ratings yet
- BAB II FitokimiaDocument8 pagesBAB II FitokimiaAryanto DedyNo ratings yet
- Dendi FitokimiaDocument3 pagesDendi FitokimiaAryanto DedyNo ratings yet
- Biodata Diri DendyDocument1 pageBiodata Diri DendyAryanto DedyNo ratings yet
- Evaluasi KapsulDocument11 pagesEvaluasi KapsulDitta Ria Arini0% (2)
- Formulasi Sediaan Gargarisma Ekstrak Biji Buah PinangxDocument74 pagesFormulasi Sediaan Gargarisma Ekstrak Biji Buah PinangxAryanto Dedy0% (1)
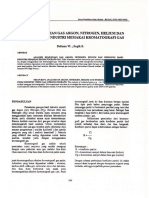
- Analisis Kemurnian Gas Argon, Nitrogen, Helium Dan Hidrogen Hasil Industri Memakai Kromatografi GasDocument4 pagesAnalisis Kemurnian Gas Argon, Nitrogen, Helium Dan Hidrogen Hasil Industri Memakai Kromatografi GasAryanto DedyNo ratings yet
- DialiserDocument5 pagesDialiserRezy Arina PutriNo ratings yet
- 150cavity Synchronization by Extended Loop in Neuraminidase of 2009 h1n1 Influenza Type A Virus A Simulation StudyDocument11 pages150cavity Synchronization by Extended Loop in Neuraminidase of 2009 h1n1 Influenza Type A Virus A Simulation StudyAryanto DedyNo ratings yet
- Formulasi Sediaan Likuid Compatibility ModeDocument25 pagesFormulasi Sediaan Likuid Compatibility ModeAryanto DedyNo ratings yet
- Flovonoid LengkuasDocument43 pagesFlovonoid LengkuasAryanto DedyNo ratings yet
- Bab IVDocument8 pagesBab IVAryanto DedyNo ratings yet
- Inti SariDocument1 pageInti SariAryanto DedyNo ratings yet
- LammpiranDocument10 pagesLammpiranAryanto DedyNo ratings yet
- Formulasi Sediaan Gargarisma Ekstrak Biji Buah PinangxDocument74 pagesFormulasi Sediaan Gargarisma Ekstrak Biji Buah PinangxAryanto Dedy0% (1)
- Kata Pengantar SantikaDocument2 pagesKata Pengantar SantikaAryanto DedyNo ratings yet
- Daftar TabelDocument1 pageDaftar TabelAryanto DedyNo ratings yet
- Bab 1-3 Fix Santika 2Document30 pagesBab 1-3 Fix Santika 2Aryanto DedyNo ratings yet
- Daftar TabelDocument1 pageDaftar TabelAryanto DedyNo ratings yet
- COVER SantikaDocument1 pageCOVER SantikaAryanto DedyNo ratings yet
- Gamavuton PembahasanDocument2 pagesGamavuton PembahasanAryanto DedyNo ratings yet
- Bab IiiDocument9 pagesBab IiiAryanto DedyNo ratings yet
- Laporan KimorsinDocument18 pagesLaporan KimorsinAryanto DedyNo ratings yet
- Bab VDocument1 pageBab VAryanto DedyNo ratings yet
- Bab IiiDocument9 pagesBab IiiAryanto DedyNo ratings yet
- UrbanDocument2 pagesUrbanAryanto DedyNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)