You might also like
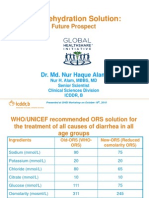
- Oral Rehydration Solution:: Future ProspectDocument48 pagesOral Rehydration Solution:: Future ProspectmustikaarumNo ratings yet
- Persistent Diarrhea-Sept2009Document43 pagesPersistent Diarrhea-Sept2009Mega Dwi PutriNo ratings yet
- International Journal of PharmacyDocument9 pagesInternational Journal of PharmacyIndra HedarNo ratings yet
- Jurnal DehidrasiDocument8 pagesJurnal DehidrasiIzza Ayudia HakimNo ratings yet
- Guidelines For Managing Acute Gastroenteritis Based On A Systematic Review of Published ResearchDocument7 pagesGuidelines For Managing Acute Gastroenteritis Based On A Systematic Review of Published ResearchnikopkunairNo ratings yet
- EBN Diarrhea OrasolDocument8 pagesEBN Diarrhea Orasolcharm_peñaNo ratings yet
- Standard WHO-ORS Versus Reduced-Osmolarity ORS in The Management of Cholera PatientsDocument6 pagesStandard WHO-ORS Versus Reduced-Osmolarity ORS in The Management of Cholera PatientsHevy Milkcha TanawaniNo ratings yet
- Recommendations: IAP Guidelines 2006 On Management of Acute DiarrheaDocument10 pagesRecommendations: IAP Guidelines 2006 On Management of Acute Diarrheaps_rajeevNo ratings yet
- Ahmed 1986Document6 pagesAhmed 1986ABCDNo ratings yet
- Ringer's Lactate vs Normal Saline for Severe Childhood DiarrheaDocument6 pagesRinger's Lactate vs Normal Saline for Severe Childhood DiarrheaVincent ScorsinniNo ratings yet
- Understanding The Use of Oral Rehydration TherapyDocument7 pagesUnderstanding The Use of Oral Rehydration TherapyJulia Intan Permata SariNo ratings yet
- Lindenschmidt 1991Document8 pagesLindenschmidt 1991aparna.cNo ratings yet
- Descripcion de Proyecto de InvestigacionDocument9 pagesDescripcion de Proyecto de InvestigacionEduardo Avalos PalaciosNo ratings yet
- R. Faruqui, H. Khanum, P. K. Bardhan, C. Mitchell, and D. A. SackDocument7 pagesR. Faruqui, H. Khanum, P. K. Bardhan, C. Mitchell, and D. A. SackJournal of Environment and Bio-SciencesNo ratings yet
- Lactobacillus Saccharomyces Boulardii: Effect of Strains and On Persistent Diarrhea in ChildrenDocument6 pagesLactobacillus Saccharomyces Boulardii: Effect of Strains and On Persistent Diarrhea in ChildrenHiteinder SharmaNo ratings yet
- Frequency of Hyponatraemia and Hypokalaemia in Malnourished Children With Acute DiarrhoeaDocument4 pagesFrequency of Hyponatraemia and Hypokalaemia in Malnourished Children With Acute DiarrhoeaRaja Bajak LautNo ratings yet
- DehidrasiDocument5 pagesDehidrasiMarlindah SNo ratings yet
- Food Based Oral Rehydration Therapy Towards A Better Choleratreatment 2329 8901 1000151Document3 pagesFood Based Oral Rehydration Therapy Towards A Better Choleratreatment 2329 8901 1000151Michael HusainNo ratings yet
- Acute Gastroenteritis in Infants and Children: Undate ArticleDocument6 pagesAcute Gastroenteritis in Infants and Children: Undate ArticlechibieNo ratings yet
- Intravenous Rehydration of Malnourished Children With Acute Gastroenteritis and Severe Dehydration: A Systematic ReviewDocument24 pagesIntravenous Rehydration of Malnourished Children With Acute Gastroenteritis and Severe Dehydration: A Systematic ReviewDina AryaniNo ratings yet
- American Journal of Gastroenterology Volume 104 Issue 10 2009 (Doi 10.1038/ajg.2009.329) Atia, Antwan N Buchman, Alan L - Oral Rehydration Solutions in Non-Cholera Diarrhea - A ReviewDocument9 pagesAmerican Journal of Gastroenterology Volume 104 Issue 10 2009 (Doi 10.1038/ajg.2009.329) Atia, Antwan N Buchman, Alan L - Oral Rehydration Solutions in Non-Cholera Diarrhea - A ReviewFadhil AbdillahNo ratings yet
- Treatment of DiarrheaDocument6 pagesTreatment of DiarrheaVictor TayoNo ratings yet
- DIAARRHEADocument23 pagesDIAARRHEARudri Pandya Shukla100% (1)
- Sucralosa y RatonesDocument13 pagesSucralosa y RatonesafamhbkNo ratings yet
- 214 FullDocument3 pages214 Fullagus fetal mein feraldNo ratings yet
- Pediatrics & Therapeutics: Congenital Chloride Losing DiarrheaDocument5 pagesPediatrics & Therapeutics: Congenital Chloride Losing Diarrheayoung mzNo ratings yet
- Randomized, Placebo-Controlled Trial of Xyloglucan and Gelose For The Treatment of Acute Diarrhea in ChildrenDocument8 pagesRandomized, Placebo-Controlled Trial of Xyloglucan and Gelose For The Treatment of Acute Diarrhea in ChildrenvalenciaNo ratings yet
- OralitDocument8 pagesOralitSanjaya lNo ratings yet
- CelluloseDocument7 pagesCellulosem waltersNo ratings yet
- Journal Reading: Ringer Lactate vs Normal Saline for Rehydration in Acute DiarrheaDocument41 pagesJournal Reading: Ringer Lactate vs Normal Saline for Rehydration in Acute Diarrheabagus aldiNo ratings yet
- "The Amrut in Dehydration": Paediatrics Department VMMC & H, KaraikalDocument38 pages"The Amrut in Dehydration": Paediatrics Department VMMC & H, KaraikalSumanth KumarNo ratings yet
- Gastroenteritis Dan MalabsorptionDocument62 pagesGastroenteritis Dan MalabsorptionDandi PremaNo ratings yet
- Studies On The Effects of Polydextrose Intake On Physiologic Functions in Chinese PeopleDocument7 pagesStudies On The Effects of Polydextrose Intake On Physiologic Functions in Chinese PeopleNhung Nguyễn Thị HồngNo ratings yet
- Diarrhoea in Children: An ApproachDocument78 pagesDiarrhoea in Children: An ApproachNP SinghNo ratings yet
- Deshidratación en Ancianos Cuidado A Largo Plazo Con Disfagia Orofaríngea 2007Document6 pagesDeshidratación en Ancianos Cuidado A Largo Plazo Con Disfagia Orofaríngea 2007Natalia BeltranNo ratings yet
- DIARRHEA Final Group 8Document65 pagesDIARRHEA Final Group 8angela marie abadillaNo ratings yet
- Management of Acute Gastroenteritis in Children: Pathophysiology in The UKDocument6 pagesManagement of Acute Gastroenteritis in Children: Pathophysiology in The UKMarnia SulfianaNo ratings yet
- Acute Gastroenteritis: Roscheyl Berg Tutor Bsn3A ' 12/14/16Document11 pagesAcute Gastroenteritis: Roscheyl Berg Tutor Bsn3A ' 12/14/16Roscheen Berg TutorNo ratings yet
- Faecal Candida and Diarrhoea: D Forbes, L Ee, P Camer-Pesci, P B WardDocument4 pagesFaecal Candida and Diarrhoea: D Forbes, L Ee, P Camer-Pesci, P B WardretnoNo ratings yet
- Approach To Acute Diarrhoea: Dr. Pankaj Kumar Singhal Govt. Medical College, KotaDocument43 pagesApproach To Acute Diarrhoea: Dr. Pankaj Kumar Singhal Govt. Medical College, KotaVandanaNo ratings yet
- Armstrong - Hydration Biomarkers and Dietary FluidDocument6 pagesArmstrong - Hydration Biomarkers and Dietary FluidAngieda SoepartoNo ratings yet
- Study of Clinical, Biochemical Evaluation and Outcome in Hypertrophic Pyloric StenosisDocument4 pagesStudy of Clinical, Biochemical Evaluation and Outcome in Hypertrophic Pyloric StenosiszapomannNo ratings yet
- Chapter - 2 - C - V-B Infectious - Diarrhea PPT AmnaDocument47 pagesChapter - 2 - C - V-B Infectious - Diarrhea PPT AmnaEmmaNo ratings yet
- Archdisch00885 0160 PDFDocument2 pagesArchdisch00885 0160 PDFKendre SantoshNo ratings yet
- AGE MarchDocument46 pagesAGE MarchJefelson Eu Palaña NahidNo ratings yet
- The Potential of Hyphaene Thebaica (Doum Palm) Fruits Extract As A Substitute For ORS in The Management of Diarrhea in Children Under Five in Sinnar State, SudanDocument7 pagesThe Potential of Hyphaene Thebaica (Doum Palm) Fruits Extract As A Substitute For ORS in The Management of Diarrhea in Children Under Five in Sinnar State, SudanSiti lestarinurhamidahNo ratings yet
- 2007 Enteral Water For Hypernatremia and Intestinal MorbidityDocument7 pages2007 Enteral Water For Hypernatremia and Intestinal MorbidityyaritzaalviarezNo ratings yet
- Transit of A Meal Through The Stomach, Small Intestine, and Colon in Normal Subjects and Its Role in The Pathogenesis of DiarrheaDocument7 pagesTransit of A Meal Through The Stomach, Small Intestine, and Colon in Normal Subjects and Its Role in The Pathogenesis of DiarrheaSmee VeselinovNo ratings yet
- Oedematous MalnutritionDocument4 pagesOedematous MalnutritionFitri Nur DiniNo ratings yet
- GASTROONTEROLOGYDocument1 pageGASTROONTEROLOGYAan WardaniNo ratings yet
- Ajcn 119925Document11 pagesAjcn 119925Rahmanu ReztaputraNo ratings yet
- Olivares2001 PDFDocument5 pagesOlivares2001 PDFEduardo Avalos PalaciosNo ratings yet
- ProbiotikDocument6 pagesProbiotikEssaLoyalLitaLestariNo ratings yet
- Azucares ReductoresDocument6 pagesAzucares ReductoresKarla Edith Rodriguez NavaNo ratings yet
- In Vivo Sorbus Decora: Original ArticleDocument8 pagesIn Vivo Sorbus Decora: Original ArticleSophea Ananoria MissionaNo ratings yet
- Farmakoterapi Sistem Pencernaan Diare Konstipasi HepatitisDocument77 pagesFarmakoterapi Sistem Pencernaan Diare Konstipasi HepatitisRefika FahruNo ratings yet
- Intravenous Rehydration of MalDocument19 pagesIntravenous Rehydration of MalDina AryaniNo ratings yet
- Lesions of the Stomach: Recognizing Hypertrophic Pyloric StenosisDocument5 pagesLesions of the Stomach: Recognizing Hypertrophic Pyloric Stenosismiracle ktmNo ratings yet
- CMC Disclaimer on Educational ContentDocument34 pagesCMC Disclaimer on Educational ContentJohn DorNo ratings yet
- Saline Therapy: Clinical Treatises on the Pathology and Therapy of Disorders of Metabolism and NutritionFrom EverandSaline Therapy: Clinical Treatises on the Pathology and Therapy of Disorders of Metabolism and NutritionNo ratings yet
- Hemangiomas and VascularMalformationsDocument10 pagesHemangiomas and VascularMalformationsRini RahmawulandariNo ratings yet
- Diagnosis Assessment CholecystitisDocument5 pagesDiagnosis Assessment CholecystitisAnonymous pJfAvlNo ratings yet
- Hemangiomas and VascularMalformationsDocument10 pagesHemangiomas and VascularMalformationsRini RahmawulandariNo ratings yet
- Ijms 038 093 PDFDocument7 pagesIjms 038 093 PDFOlpinNo ratings yet
- Tropmed 82 412Document3 pagesTropmed 82 412OlpinNo ratings yet
- 5666 11015 1 SM PDFDocument8 pages5666 11015 1 SM PDFGloria Kristina LikoNo ratings yet
- Efficacy of A New Hypotonic Oral Rehydration Solution Containing Zinc and Prebiotics in The Treatment of Childhood Acute Diarrhea: A Randomized Controlled TrialDocument6 pagesEfficacy of A New Hypotonic Oral Rehydration Solution Containing Zinc and Prebiotics in The Treatment of Childhood Acute Diarrhea: A Randomized Controlled TrialOlpinNo ratings yet
- Cover Biokimia PDFDocument1 pageCover Biokimia PDFDaisy LoussierNo ratings yet
- BLT 10 075986Document7 pagesBLT 10 075986Novriman LiviaNo ratings yet
- New Developments in Management of Meningioma 2329 6771 1000135Document9 pagesNew Developments in Management of Meningioma 2329 6771 1000135OlpinNo ratings yet
- 1intracranial Meningioma PDFDocument8 pages1intracranial Meningioma PDFOlpinNo ratings yet
- Neo PhysiologyDocument6 pagesNeo PhysiologyLydia Angelia YanitaNo ratings yet
- Reviewing SRHR in Asian DisastersDocument67 pagesReviewing SRHR in Asian DisastersOlpinNo ratings yet
- In Vitro Fluoride Toxicity in Human Spermatozoa - Reproductive Toxicology, Vol. 8, No. 2, Pp. 155-159, 1994 PDFDocument5 pagesIn Vitro Fluoride Toxicity in Human Spermatozoa - Reproductive Toxicology, Vol. 8, No. 2, Pp. 155-159, 1994 PDFStefania WidyaNo ratings yet
- Brain Tumors - KY Cancer RegistryDocument45 pagesBrain Tumors - KY Cancer RegistryMohammad Galih PratamaNo ratings yet
- Rehabilitation Program For InmatesDocument37 pagesRehabilitation Program For InmatesChing DialomaNo ratings yet
- Osteomyelitis: Osteomyelitis Is Infection in The Bone. Osteomyelitis Can Occur in InfantsDocument4 pagesOsteomyelitis: Osteomyelitis Is Infection in The Bone. Osteomyelitis Can Occur in Infantstiban_07No ratings yet
- Riwayat Pendidikan Riwayat PekerjaanDocument36 pagesRiwayat Pendidikan Riwayat PekerjaanRam PrototokonNo ratings yet
- PDPHDocument19 pagesPDPHcardiacanesthesiaNo ratings yet
- Southampton Grading SystemDocument5 pagesSouthampton Grading SystemswestyNo ratings yet
- Hexa Health guides patients through surgery processDocument2 pagesHexa Health guides patients through surgery processSarvesh KashyapNo ratings yet
- Objectives and Research Methodology Chapter on Stress Among Women in IT SectorDocument38 pagesObjectives and Research Methodology Chapter on Stress Among Women in IT SectorShreya MuralidharanNo ratings yet
- Progressive Balbar Palsy: Dr. Mohamed Ali 3 Year MD IM ResidentDocument15 pagesProgressive Balbar Palsy: Dr. Mohamed Ali 3 Year MD IM ResidentMohamed AliNo ratings yet
- HEALTH - REAC - 4 - Physicians by CategoriesDocument44 pagesHEALTH - REAC - 4 - Physicians by CategoriesAbhinav NaiduNo ratings yet
- Medical Billing ProcessDocument24 pagesMedical Billing ProcessNajamHass100% (5)
- NHS Patient Safety SyllabusDocument22 pagesNHS Patient Safety SyllabusMubeenRahmanNo ratings yet
- Fat Burner: Fitzoye Nutrition IntroducingDocument6 pagesFat Burner: Fitzoye Nutrition IntroducingrajeshNo ratings yet
- CMC Vellore Summer Admission Bulletin 2020 Revised 16 Nov 2020Document58 pagesCMC Vellore Summer Admission Bulletin 2020 Revised 16 Nov 2020Allen ChrysoNo ratings yet
- Case Study Risk ManagementDocument2 pagesCase Study Risk ManagementQueen SeñalistaNo ratings yet
- Factories Act 1948 provisions for worker safetyDocument16 pagesFactories Act 1948 provisions for worker safetyTheeppori SomanNo ratings yet
- Healthy Delights Magazine Filled With 42 Quick RecipesDocument8 pagesHealthy Delights Magazine Filled With 42 Quick RecipesYasser NazmyNo ratings yet
- Soal Lokasi KIK - 2Document2 pagesSoal Lokasi KIK - 2novida nainggolanNo ratings yet
- WPH VMO Directory1Document56 pagesWPH VMO Directory1Ragupathi MNo ratings yet
- Appointment Letters Independent DirectorsDocument62 pagesAppointment Letters Independent DirectorsArudra KumarNo ratings yet
- Pneumonia AnswersDocument5 pagesPneumonia AnswersColeen Mae CamaristaNo ratings yet
- Safety Data Sheet Belzona® 9111 (Cleaner/Degreaser) : 1. Identification of The Substance/Preparation and The CompanyDocument7 pagesSafety Data Sheet Belzona® 9111 (Cleaner/Degreaser) : 1. Identification of The Substance/Preparation and The CompanyPetraindo Jaya AbadiNo ratings yet
- Homeopathy CuresDocument18 pagesHomeopathy CureschampakNo ratings yet
- Government of NCT of Delhi Delhi Subordinate Services Selection Board Fc-18, Institutional Area, Karkardooma, DelhiDocument3 pagesGovernment of NCT of Delhi Delhi Subordinate Services Selection Board Fc-18, Institutional Area, Karkardooma, DelhiVivekRawalNo ratings yet
- Artificial RespirationDocument3 pagesArtificial RespirationRenju JoseNo ratings yet
- Well Fact Sheet: Suitability of Water For Livestock Fact SheetDocument2 pagesWell Fact Sheet: Suitability of Water For Livestock Fact SheetHill County Conservation DistrictNo ratings yet
- Module 1: Disability, Inequality, and InclusionDocument25 pagesModule 1: Disability, Inequality, and InclusionAuberon Jeleel OdoomNo ratings yet
- Aba 2506Document7 pagesAba 2506Mutiso BrianNo ratings yet
- List of Chyawanprash Manufacturers in IndiaDocument3 pagesList of Chyawanprash Manufacturers in Indiaplacementducat63No ratings yet
- Liver Cirrhosis: Causes, Complications and ManagementDocument55 pagesLiver Cirrhosis: Causes, Complications and ManagementAnonymous vUEDx8100% (1)