You might also like
- Buku Gizi Buruk I 2011 - 2 PDFDocument41 pagesBuku Gizi Buruk I 2011 - 2 PDFNicko Erdy Kusuma100% (8)
- Buku Saku - Lima Langkah Tuntaskan Diare - Depkes Ri 2011Document40 pagesBuku Saku - Lima Langkah Tuntaskan Diare - Depkes Ri 2011familyman8083% (6)
- singkat dokumen tentang infeksi menular seksualDocument42 pagessingkat dokumen tentang infeksi menular seksualGede GiriNo ratings yet
- PPK-edit FINAL PDFDocument566 pagesPPK-edit FINAL PDFNurul Laili NahliaNo ratings yet
- PPK-edit FINAL PDFDocument566 pagesPPK-edit FINAL PDFNurul Laili NahliaNo ratings yet
- Status MataDocument5 pagesStatus MataAnna Hafeezah ZahrahNo ratings yet
- HEMATOKEZIADocument58 pagesHEMATOKEZIAAnonymous 7xR3ymgNo ratings yet
- Status Luka BakarDocument17 pagesStatus Luka BakarBenny KurniawanNo ratings yet
- Kegawatdaruratan THTKL 1 PDFDocument20 pagesKegawatdaruratan THTKL 1 PDFBudi SetyanugrahaNo ratings yet
- Form 1aDocument2 pagesForm 1aRoni Dwi HerdiantoNo ratings yet
- Contoh Notulen RapatDocument7 pagesContoh Notulen RapatlusyeNo ratings yet
- Dokter Layanan Primer 2Document17 pagesDokter Layanan Primer 2Dina RyantiNo ratings yet
- EIMED PAPDI Kegawatdaruratan Penyakit DalamDocument6 pagesEIMED PAPDI Kegawatdaruratan Penyakit DalamAnneAyushaNo ratings yet
- OBGIN RSUP Dr. M. DJAMIL PADANGDocument48 pagesOBGIN RSUP Dr. M. DJAMIL PADANGprimaindra27No ratings yet
- Tinpus Skin DeglovingDocument14 pagesTinpus Skin DeglovingAhimsa MartawigunaNo ratings yet
- Presentasi Kasus - Trauma Wajah - FK UIN Jakarta Oktober 2017Document59 pagesPresentasi Kasus - Trauma Wajah - FK UIN Jakarta Oktober 2017Irma Sari Muliadi100% (1)
- KMK No. HK.01.07-MENKES-1970-2022 TTG Perubahan TTG Formularium Nasional-SignedDocument284 pagesKMK No. HK.01.07-MENKES-1970-2022 TTG Perubahan TTG Formularium Nasional-SignedfitriahNo ratings yet
- Laporan KasusDocument59 pagesLaporan KasusNova Romanggwandi RumbinoNo ratings yet
- PREEKLAMPSIADocument36 pagesPREEKLAMPSIAClever ImaniaNo ratings yet
- Referat Tinea Versikolor UnhasDocument7 pagesReferat Tinea Versikolor Unhasjimmypatabang10No ratings yet
- 8 Jurus SamuraiDocument280 pages8 Jurus SamuraiRifki KhairulNo ratings yet
- Jadwal Imunisasi 2006Document2 pagesJadwal Imunisasi 2006Meirhae Tetap CeriiaNo ratings yet
- Imunisasi DewasaDocument12 pagesImunisasi Dewasatiwiprasetya100% (1)
- OFTALMOLOGIDocument4 pagesOFTALMOLOGIRyan Haryana DarajatunNo ratings yet
- HerniaScrotalisDocument8 pagesHerniaScrotalisDyo ResnaNo ratings yet
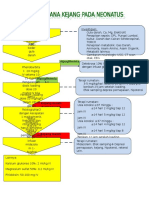
- Tatalaksana Kejang NeonatusDocument1 pageTatalaksana Kejang NeonatusMerlyn_RumtheNo ratings yet
- Kasus Otitis Media AkutDocument12 pagesKasus Otitis Media AkutElya AulanivaNo ratings yet
- Kasus EsofagitisDocument16 pagesKasus EsofagitisAjeng SalsabillaNo ratings yet
- Trauma Ubur-uburDocument28 pagesTrauma Ubur-uburGerbong 5 ArticulatioNo ratings yet
- DIAGNOSISDocument19 pagesDIAGNOSISViskaNo ratings yet
- BEDAH MINOR OPTIMALDocument17 pagesBEDAH MINOR OPTIMALKahubbi Fatimah Wa'aliyNo ratings yet
- Ketuban Pecah Dini Dan Infeksi IntrapartumDocument4 pagesKetuban Pecah Dini Dan Infeksi IntrapartumRizka Yunita0% (1)
- STUNTING DI INDONESIADocument10 pagesSTUNTING DI INDONESIAMia KimNo ratings yet
- MR Kardiologi FK UnhasDocument75 pagesMR Kardiologi FK UnhaslucyishakNo ratings yet
- Kasus IntoksikasiDocument40 pagesKasus IntoksikasiDevi YuliantiNo ratings yet
- BPPVDocument23 pagesBPPVElfon PratamaNo ratings yet
- Tonsilitis KronisDocument49 pagesTonsilitis KronisHannisa SandhaNo ratings yet
- ILEUS PARALITIKDocument41 pagesILEUS PARALITIKDiandhara NuryadinNo ratings yet
- Hasil Survey Kedua Minat Wahana Internsip Februari 2017Document12 pagesHasil Survey Kedua Minat Wahana Internsip Februari 2017Ikram Ikram100% (1)
- Letak LintangDocument36 pagesLetak LintangErwin SiregarNo ratings yet
- KRITISDocument5 pagesKRITISAdlina Karimina HusnaNo ratings yet
- RADIKULOPATIDocument39 pagesRADIKULOPATIAnonymous ChK10iwGxNo ratings yet
- Dokter SpesialisDocument11 pagesDokter SpesialisDody ChandraNo ratings yet
- Diagnosis Dan Tata Laksana Ensefalitis Herpes SimpleksDocument3 pagesDiagnosis Dan Tata Laksana Ensefalitis Herpes SimpleksaandakuNo ratings yet
- (Case) Hemiparese Sinistra Tipe SpastikDocument35 pages(Case) Hemiparese Sinistra Tipe Spastikcookies landNo ratings yet
- Kasus DHF Grade 2Document9 pagesKasus DHF Grade 2Alif AdlanNo ratings yet
- Retensio Urine Et Causa Striktur UretraDocument43 pagesRetensio Urine Et Causa Striktur UretraNovia Rizki AmaliaNo ratings yet
- CRS HepatomaDocument46 pagesCRS HepatomaalgutNo ratings yet
- Laporan Kasus Koas RadiologiDocument48 pagesLaporan Kasus Koas Radiologirina trisnaningNo ratings yet
- Kapita Selekta Kedokteran Edisi IV Jilid 1Document2 pagesKapita Selekta Kedokteran Edisi IV Jilid 1فرجني موغNo ratings yet
- Daftar Mahasiswa UnudDocument53 pagesDaftar Mahasiswa Unudsania_salsabila0% (1)
- Textbook Reading PAPDI (339 Anemia Hemolitik Imun) - DikonversiDocument30 pagesTextbook Reading PAPDI (339 Anemia Hemolitik Imun) - DikonversiSumanjaya PratamaNo ratings yet
- TONSILITIS KRONIK DAN PRESTASI BELAJARDocument5 pagesTONSILITIS KRONIK DAN PRESTASI BELAJARDewi ArdianaNo ratings yet
- Compound Miopia AstigmatDocument21 pagesCompound Miopia AstigmatrezkyNo ratings yet
- Lamaran Dokter UmumDocument24 pagesLamaran Dokter UmumAkbar AkbarNo ratings yet
- BEDAH PLASTIKDocument13 pagesBEDAH PLASTIKpivvNo ratings yet
- Cover LevyDocument2 pagesCover LevylevyazkaNo ratings yet
- PPK Tindakan HemispicaDocument2 pagesPPK Tindakan HemispicaWadhe Omara TobingNo ratings yet
- RumusDocument3 pagesRumusLinda WaromiNo ratings yet
- EYE DISEASEDocument67 pagesEYE DISEASEJulianda EpriantiNo ratings yet
- Kote Noordhianta, DR., SP - THT-KL., M.kes Tatalaksana EpistaksisDocument30 pagesKote Noordhianta, DR., SP - THT-KL., M.kes Tatalaksana Epistaksisageng01101750% (1)
- MODUL HIDUNG EPISTAKSIS (Presentasi)Document30 pagesMODUL HIDUNG EPISTAKSIS (Presentasi)kucingmeong1922No ratings yet
- Menghentikan Perdarahan Hidung-2Document33 pagesMenghentikan Perdarahan Hidung-2Delya SukmaNo ratings yet
- CRS Epistaksis Kavum Nasi Dextra Dan SinistraDocument41 pagesCRS Epistaksis Kavum Nasi Dextra Dan SinistraMatahari LingkarNo ratings yet
- EPISTAKSISDocument26 pagesEPISTAKSISNova AweiNo ratings yet
- EPISTAKSISDocument23 pagesEPISTAKSISDonna PatandiananNo ratings yet
- Bahayanarkotikaterhadapkesehatan 111125003259 Phpapp02Document20 pagesBahayanarkotikaterhadapkesehatan 111125003259 Phpapp02Gede GiriNo ratings yet
- 60 117 1 SMDocument12 pages60 117 1 SMNurfadhilahNo ratings yet
- Refleksi Kasus Jiwa 2014 DR - BasiranDocument7 pagesRefleksi Kasus Jiwa 2014 DR - BasiranGede GiriNo ratings yet
- CLINICAL MENTORING 7 MANAJEMEN NYERI KRONIK OLEH Dr. DARMA IMRAN SP.S K PDFDocument28 pagesCLINICAL MENTORING 7 MANAJEMEN NYERI KRONIK OLEH Dr. DARMA IMRAN SP.S K PDFGede GiriNo ratings yet
- Anti Tetanus PDFDocument6 pagesAnti Tetanus PDFnyuwwchocolavaNo ratings yet
- 60 117 1 SMDocument12 pages60 117 1 SMNurfadhilahNo ratings yet
- Satelit Simposium 22.1 Home Care Oleh Prof. Dr. Dr. Siti Setiati SPDocument35 pagesSatelit Simposium 22.1 Home Care Oleh Prof. Dr. Dr. Siti Setiati SPGede GiriNo ratings yet
- UU No 23 Tahun 2003 PERLINDUNGAN ANAKDocument14 pagesUU No 23 Tahun 2003 PERLINDUNGAN ANAKRudi Pradisetia SudirdjaNo ratings yet
- Surat Pernyataan Belum Pernah DimuatDocument1 pageSurat Pernyataan Belum Pernah DimuatGede GiriNo ratings yet
- Daftar Isi & Kata PengantarDocument2 pagesDaftar Isi & Kata PengantarGede GiriNo ratings yet
- Cover Dan Lembar PengesahanDocument2 pagesCover Dan Lembar PengesahanGede GiriNo ratings yet
- @3523170 Kda Tambakboyo 2013Document79 pages@3523170 Kda Tambakboyo 2013Gede GiriNo ratings yet
- Daftar Isi & Kata PengantarDocument2 pagesDaftar Isi & Kata PengantarGede GiriNo ratings yet
- NSPK PMKS PSKS PERMENSOS No 08 TH 2012Document29 pagesNSPK PMKS PSKS PERMENSOS No 08 TH 2012Noor HalizaNo ratings yet
- BiodataDocument2 pagesBiodataGede GiriNo ratings yet
- Rhematoid Heart Disease With Mitral and Tricuspid StenosisDocument56 pagesRhematoid Heart Disease With Mitral and Tricuspid StenosisGede GiriNo ratings yet
- Surat Keterangan Sehat UKDI - STRDocument4 pagesSurat Keterangan Sehat UKDI - STRcyelzNo ratings yet
- Lapsus Rhd+mitral Stenosis+trikuspid StenosisDocument28 pagesLapsus Rhd+mitral Stenosis+trikuspid StenosisGede GiriNo ratings yet
- Statistik Daerah Kecamatan Tambakboyo Tahun 2014 PDFDocument42 pagesStatistik Daerah Kecamatan Tambakboyo Tahun 2014 PDFGede GiriNo ratings yet
- Sop NurjayaDocument3 pagesSop NurjayaGede GiriNo ratings yet
- METODE MEMBAYAR DOKTERDocument65 pagesMETODE MEMBAYAR DOKTERHida Nur Hidayah DemakNo ratings yet
- Case Bell S Palsy Rila PutriDocument26 pagesCase Bell S Palsy Rila PutriGede GiriNo ratings yet
- Pengumuman STR InternsipDocument1 pagePengumuman STR InternsipDeby PurwantoNo ratings yet