You might also like
- Cures, Health & Wellbeing PDFDocument1,741 pagesCures, Health & Wellbeing PDFkitty katNo ratings yet
- Syllabus ElectrotherapyDocument4 pagesSyllabus ElectrotherapySYED ALI HUSSAINNo ratings yet
- Health AssessmentDocument30 pagesHealth AssessmentWeng RamojalNo ratings yet
- Drugs and DosagesDocument30 pagesDrugs and DosagesvanessaNo ratings yet
- Assessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsFrom EverandAssessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsNo ratings yet
- Acupuncture: Halos, Heredia, Herejias, HicarteDocument45 pagesAcupuncture: Halos, Heredia, Herejias, Hicarteshelbyheredia0% (1)
- Wound Management Guide DigitalDocument48 pagesWound Management Guide DigitalBrian NiuNo ratings yet
- Demonstrate: Pain Coping TechniquesDocument4 pagesDemonstrate: Pain Coping TechniquesMae Therese B. MAGNO100% (1)
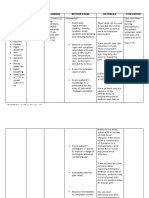
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument5 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationArian May MarcosNo ratings yet
- Acute Pain Nursing Diagnosis & Care Plan - NurseslabsDocument1 pageAcute Pain Nursing Diagnosis & Care Plan - NurseslabsShimaa Al SiyabiNo ratings yet
- Chapter 39 Pain Management in ChildrenDocument3 pagesChapter 39 Pain Management in ChildrenAllyssa Mackinnon0% (1)
- Epidural AnalgesiaDocument16 pagesEpidural AnalgesiaspreeasNo ratings yet
- Pain Assessment and ManagementDocument37 pagesPain Assessment and ManagementRNdrei dela Cruz100% (3)
- Pain Assessment and Management: Lecturer: Sharon A. Guillo Date: TimeDocument31 pagesPain Assessment and Management: Lecturer: Sharon A. Guillo Date: Timesharon alvarezNo ratings yet
- Nursing Care Plan - AnxietyDocument1 pageNursing Care Plan - AnxietyPauPau100% (1)
- Principles of Pain Management: Pediatric GuideDocument2 pagesPrinciples of Pain Management: Pediatric Guideblaziken123No ratings yet
- Acute Pain in CatsDocument10 pagesAcute Pain in CatsLINDA BELMONTNo ratings yet
- 10 1016@j Mpaic 2019 03 003 PDFDocument4 pages10 1016@j Mpaic 2019 03 003 PDFsondiNo ratings yet
- 10 1016@j Mpaic 2019 03 003 PDFDocument4 pages10 1016@j Mpaic 2019 03 003 PDFHerold23No ratings yet
- 23 - RA-Dmytro-Ped Pain - HP WordDocument10 pages23 - RA-Dmytro-Ped Pain - HP WordaldybebikaNo ratings yet
- Lecture 6 Pain Management in Children by Pharmacological and NonDocument25 pagesLecture 6 Pain Management in Children by Pharmacological and NonRubinaNo ratings yet
- Nurses TrainingDocument18 pagesNurses TrainingpriskayoviNo ratings yet
- N11 Nursing Foundations IiDocument4 pagesN11 Nursing Foundations IiAlec Xavier MirandaNo ratings yet
- Pain AssessmentDocument22 pagesPain AssessmentpuchioNo ratings yet
- Post Operative Pain Management in Paediatric Patients: Dr. R. P. GehdooDocument9 pagesPost Operative Pain Management in Paediatric Patients: Dr. R. P. GehdooT RonaskyNo ratings yet
- Pain Measurement 2Document6 pagesPain Measurement 2Shahnawaz ShahNo ratings yet
- Analgesia in The Emergency Department - IAEM Clinical GuidelineDocument14 pagesAnalgesia in The Emergency Department - IAEM Clinical GuidelineEumed.orgNo ratings yet
- Current Practice and Recent Advances in Pediatric Pain ManagementDocument15 pagesCurrent Practice and Recent Advances in Pediatric Pain ManagementSyane TitaleyNo ratings yet
- A Guide To Pain Assessment and ManagementDocument14 pagesA Guide To Pain Assessment and ManagementKitesaMedeksaNo ratings yet
- Healthcare Tech Letters - 2018 - Subramaniam - Scope of Physiological and Behavioural Pain Assessment Techniques inDocument6 pagesHealthcare Tech Letters - 2018 - Subramaniam - Scope of Physiological and Behavioural Pain Assessment Techniques injoelruizmaNo ratings yet
- Epidemiology and Definition: o Most Common Locations: o Acute PainDocument4 pagesEpidemiology and Definition: o Most Common Locations: o Acute PainJudy Ignacio EclarinoNo ratings yet
- Paediatric Handbook - (CHAPTER 3 Pain Management)Document19 pagesPaediatric Handbook - (CHAPTER 3 Pain Management)Cherry ZengNo ratings yet
- Adult Non Verbal Pain Scale UpdatedDocument15 pagesAdult Non Verbal Pain Scale UpdatedGay PopNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care Planlowell cerezoNo ratings yet
- Assessment and Management of PainDocument75 pagesAssessment and Management of PainprashantNo ratings yet
- Nurses Role in Pain Assessment & Pain ManagementDocument32 pagesNurses Role in Pain Assessment & Pain ManagementroyNo ratings yet
- Pain Assessment, Reassessment and Management, Grief and Bereavement, End of LIfe CareDocument26 pagesPain Assessment, Reassessment and Management, Grief and Bereavement, End of LIfe Carewilliam turquezaNo ratings yet
- Assessing Pain Using Patient Reported Outcome MeasDocument3 pagesAssessing Pain Using Patient Reported Outcome MeasAndrésNo ratings yet
- 3 Peran Perawat Dalam Managemen Nyeri-1Document55 pages3 Peran Perawat Dalam Managemen Nyeri-1Anonymous PBDr0ONo ratings yet
- 10-Powell+etal-V2 2 PDFDocument12 pages10-Powell+etal-V2 2 PDFPenelopeShamNo ratings yet
- Pain ScaleDocument1 pagePain Scaleyordanos getachewNo ratings yet
- Berihun CPRST Pain AssessmentDocument23 pagesBerihun CPRST Pain AssessmentAhmed YunusNo ratings yet
- Pain AssessmentDocument15 pagesPain AssessmentAvash ZhaNo ratings yet
- Assessment of Chronic Pain: Domains, Methods, and MechanismsDocument11 pagesAssessment of Chronic Pain: Domains, Methods, and MechanismsDana LebadaNo ratings yet
- Instrumen Penilaian Nyeri Pada Anak Dengan Gangguan Kognitif: ADocument9 pagesInstrumen Penilaian Nyeri Pada Anak Dengan Gangguan Kognitif: AAkun DownloadNo ratings yet
- Validation of The Numerical Rating Scale For Pain Intensity and Unpleasantness in Pediatric Acute Postoperative Pain: Sensitivity To Change Over TimeDocument11 pagesValidation of The Numerical Rating Scale For Pain Intensity and Unpleasantness in Pediatric Acute Postoperative Pain: Sensitivity To Change Over Timefahmi zalimuNo ratings yet
- Materi Pelatihan Manajemen Nyeri 2019Document52 pagesMateri Pelatihan Manajemen Nyeri 2019Iman Muhamad FirmansyahNo ratings yet
- Pain Measurement in Patients With Low Back PainDocument9 pagesPain Measurement in Patients With Low Back PainAnakagung Vinna ParamitaNo ratings yet
- 2009 Pain Assessment and ManagementDocument22 pages2009 Pain Assessment and ManagementErnawa RikaNo ratings yet
- Bagas Anggara Permadi Bab IIDocument106 pagesBagas Anggara Permadi Bab IIInna Nur Fitri DahliyantiNo ratings yet
- Revised: 06/08: PurposeDocument8 pagesRevised: 06/08: PurposecakNo ratings yet
- 8.3 Pain PresentationDocument24 pages8.3 Pain PresentationEstela Such GilNo ratings yet
- 1 s2.0 S1094919422000457 MainDocument29 pages1 s2.0 S1094919422000457 MainRafael Silva CortésNo ratings yet
- 3-3 Pain Assessment in ChildrenDocument6 pages3-3 Pain Assessment in ChildrenMohammed TariqNo ratings yet
- The Measurement of Pain in Patients With Trigeminal NeuralgiaDocument5 pagesThe Measurement of Pain in Patients With Trigeminal NeuralgiaShellyanaCindyNo ratings yet
- Heart Clinic: Alternative Learning System Related Learning ExperienceDocument8 pagesHeart Clinic: Alternative Learning System Related Learning ExperienceEdson John DemayoNo ratings yet
- Pain Assessment in Older Adults Post Viewing ReportDocument2 pagesPain Assessment in Older Adults Post Viewing ReportLiam HenryNo ratings yet
- .Dolor Neonato TradDocument10 pages.Dolor Neonato TradAsdrubal MontañoNo ratings yet
- Form Pengkajian KosonganDocument34 pagesForm Pengkajian KosonganYurike OliviaNo ratings yet
- Goals and Outcomes: Acute Pain Is Characterized by The Following Signs and SymptomsDocument5 pagesGoals and Outcomes: Acute Pain Is Characterized by The Following Signs and SymptomsCyril Jane Caanyagan AcutNo ratings yet
- Nyeri Pada AnakDocument34 pagesNyeri Pada AnakyoelbagusNo ratings yet
- Final Post TestDocument23 pagesFinal Post TestJoanne Bernadette AguilarNo ratings yet
- Quizz ClinicDocument3 pagesQuizz ClinicKia MadineNo ratings yet
- Pain Assesment in NeonatesDocument7 pagesPain Assesment in Neonatesfuka priesleyNo ratings yet
- Coping Resources and Affective Responses: Assessment InterviewDocument6 pagesCoping Resources and Affective Responses: Assessment Interviewrahtu suzi ameliaNo ratings yet
- Guidelines For Counselling English PDFDocument16 pagesGuidelines For Counselling English PDFBrian NiuNo ratings yet
- Derma Sciences Product GuideDocument36 pagesDerma Sciences Product GuideBrian NiuNo ratings yet
- Book2 Wound Dressing GuideDocument51 pagesBook2 Wound Dressing GuideBrian Niu100% (1)
- Puprevman Bps Mar09Document40 pagesPuprevman Bps Mar09Brian NiuNo ratings yet
- Wound Care Guide by Wound TypeDocument1 pageWound Care Guide by Wound TypeBrian NiuNo ratings yet
- Wound Management Formulary Bedfordshire November 2010Document67 pagesWound Management Formulary Bedfordshire November 2010Brian NiuNo ratings yet
- Intro Anesthesia 2016 EmergencyDocument14 pagesIntro Anesthesia 2016 EmergencyBrian NiuNo ratings yet
- Intro Anesthesia 2016 AirwayDocument39 pagesIntro Anesthesia 2016 AirwayBrian NiuNo ratings yet
- Intro Anesthesia 2016 Pain RegionalDocument29 pagesIntro Anesthesia 2016 Pain RegionalBrian NiuNo ratings yet
- Intro Anesthesia 2016 PreopDocument33 pagesIntro Anesthesia 2016 PreopBrian NiuNo ratings yet
- Oleia Topical Oil Clinical Trial On Safety by DR Catherine LegaspiDocument17 pagesOleia Topical Oil Clinical Trial On Safety by DR Catherine LegaspiOleiaNo ratings yet
- Lower Back PainDocument18 pagesLower Back PainmeganNo ratings yet
- Your FibromyalgiaDocument3 pagesYour FibromyalgiaLGNo ratings yet
- Newapproachestopain Management: Orrett E. OgleDocument10 pagesNewapproachestopain Management: Orrett E. OgleNajeeb UllahNo ratings yet
- IV. Modul 10 - Pengelolaan NyeriDocument97 pagesIV. Modul 10 - Pengelolaan NyeriGrace Noviyanthi SinambelaNo ratings yet
- Competitive Assessment and Market Entry Study of Devil's Claw in The USADocument90 pagesCompetitive Assessment and Market Entry Study of Devil's Claw in The USAAnonymous 5i7xlopj8No ratings yet
- Daño Hepatico Manejo DolorDocument6 pagesDaño Hepatico Manejo DolorAngélica Valenzuela AndrighiNo ratings yet
- JM DrugDocument3 pagesJM DrugVerdie B. NgayanNo ratings yet
- Wildlife Rehabilitation Study GuideDocument8 pagesWildlife Rehabilitation Study GuideStacie BoothNo ratings yet
- Surgical Ward Drug StudyDocument23 pagesSurgical Ward Drug StudyKatherine May F. LloritoNo ratings yet
- Chapter 1 Perioperative NursingDocument19 pagesChapter 1 Perioperative NursingKathleen Dela CruzNo ratings yet
- Postoperative Pain Control: Veerabhadram Garimella, MD, MRCS Christina Cellini, MDDocument6 pagesPostoperative Pain Control: Veerabhadram Garimella, MD, MRCS Christina Cellini, MDEva Oktavianti NainggolanNo ratings yet
- Pathophysiology of OsteoarthritisDocument41 pagesPathophysiology of OsteoarthritisghaziaNo ratings yet
- Integrated Therapeutics IiiDocument15 pagesIntegrated Therapeutics IiiSalahadinNo ratings yet
- Introduce The OTC Pain RelieversDocument9 pagesIntroduce The OTC Pain RelieversNam's ThhanhNo ratings yet
- Concept Map PT 1Document1 pageConcept Map PT 1api-657741346No ratings yet
- Presentation On: Beximco PharmaDocument37 pagesPresentation On: Beximco PharmaToukir Ahmed100% (1)
- Digital Paper TrailDocument4 pagesDigital Paper Trailapi-432788054No ratings yet
- Postoperative Analgesia in Modified Radical Mastectomy Patients After Instillation of Bupivacaine Through Surgical Drains-1.en - IdDocument23 pagesPostoperative Analgesia in Modified Radical Mastectomy Patients After Instillation of Bupivacaine Through Surgical Drains-1.en - Idsatria divaNo ratings yet
- Remifentanil Versus Propofol/Fentanyl Combination in Procedural Sedation For Dislocated Shoulder Reduction A Clinical TrialDocument5 pagesRemifentanil Versus Propofol/Fentanyl Combination in Procedural Sedation For Dislocated Shoulder Reduction A Clinical TrialerinNo ratings yet
- What Are The Therapeutic Classes of DrugsDocument3 pagesWhat Are The Therapeutic Classes of DrugsFrank GomesNo ratings yet
- Jper 21-0153Document9 pagesJper 21-0153sasi dharanNo ratings yet
- Unit 9 Taking About Symtoms + Unit 13 Family MedicineDocument2 pagesUnit 9 Taking About Symtoms + Unit 13 Family MedicineThuy AnhNo ratings yet
- Rle NCMB 314-M2-Cu6Document6 pagesRle NCMB 314-M2-Cu6Jordz PlaciNo ratings yet
- Alur Manajemen Nyeri Rumah SakitDocument45 pagesAlur Manajemen Nyeri Rumah SakitRadit NasillaNo ratings yet