You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Clinical Features, Etiologies, and Outcomes in Adult Patients WithDocument13 pagesClinical Features, Etiologies, and Outcomes in Adult Patients Withagarrido2No ratings yet
- No. Name Position Monday Administration: Alternative Work Arrangement Jose C. Payumo Jr. Memorial High SchoolDocument35 pagesNo. Name Position Monday Administration: Alternative Work Arrangement Jose C. Payumo Jr. Memorial High SchoolJeremy Desoyo TorresNo ratings yet
- Table 1 Classification and Staging Systems For AKIDocument1 pageTable 1 Classification and Staging Systems For AKIAnityo NugrohoNo ratings yet
- Active Cycle of Breathing TechniqueDocument2 pagesActive Cycle of Breathing TechniqueKurniawaty SupriyadiNo ratings yet
- Henoch Schonlein Purpura GuidelineDocument12 pagesHenoch Schonlein Purpura GuidelinewenyinriantoNo ratings yet
- Top10ReasonsToUseIVUS PDFDocument71 pagesTop10ReasonsToUseIVUS PDFDiana PânteaNo ratings yet
- Case Presentation ScabiesDocument26 pagesCase Presentation Scabieshardi auliaNo ratings yet
- Clinical Genetics: General Aspects and Laboratory DiagnosticsDocument14 pagesClinical Genetics: General Aspects and Laboratory DiagnosticsKinga-Borbála GagyiNo ratings yet
- (2020) Pearls and Pitfalls of Interpretation in CT ColonographyDocument9 pages(2020) Pearls and Pitfalls of Interpretation in CT ColonographyChristian ToalongoNo ratings yet
- (Medical Psychiatry 29) Borwin Bandelow, Dan J. Stein - Social Anxiety Disorder-Marcel Dekker (2004) PDFDocument347 pages(Medical Psychiatry 29) Borwin Bandelow, Dan J. Stein - Social Anxiety Disorder-Marcel Dekker (2004) PDFmaria100% (1)
- LoadVoucher AspxDocument4 pagesLoadVoucher AspxEdnalyn CasasNo ratings yet
- @ (White Paper Cut-Off) QUS 0202 FinalDocument13 pages@ (White Paper Cut-Off) QUS 0202 FinalHajjab AnasNo ratings yet
- Bayabas: Instructions For GuavaDocument2 pagesBayabas: Instructions For GuavadorothypearlNo ratings yet
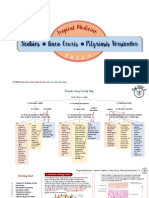
- Scabies Tinea Cruris Pityriasis Versicolor: Semangat!Document11 pagesScabies Tinea Cruris Pityriasis Versicolor: Semangat!Fitriah Nur SyamiatiNo ratings yet
- Public Health Department, MaharashtraDocument6 pagesPublic Health Department, MaharashtraNDTVNo ratings yet
- 14 Factitious Disorders and MalingeringDocument13 pages14 Factitious Disorders and Malingeringkrysdana22100% (1)
- Allergies or Food Intolerances.: Therapeutic DietDocument3 pagesAllergies or Food Intolerances.: Therapeutic DietBryan Mae H. DegorioNo ratings yet
- List of Top Level Categories: CHAPTER 01 Certain Infectious or Parasitic DiseasesDocument148 pagesList of Top Level Categories: CHAPTER 01 Certain Infectious or Parasitic Diseasesျပည္ စိုးNo ratings yet
- Ship Captain's Medical Guide - 22nd EdDocument224 pagesShip Captain's Medical Guide - 22nd EdcelmailenesNo ratings yet
- What Is An Ear InfectionDocument4 pagesWhat Is An Ear Infectionapi-236387116No ratings yet
- Mastectomy: Presenter: DR Janardhan T Post GraduateDocument49 pagesMastectomy: Presenter: DR Janardhan T Post GraduateASHUTOSH KUMARNo ratings yet
- Icd-10 Oktober 2021Document9 pagesIcd-10 Oktober 2021Nia KurniawatiNo ratings yet
- Conjunctivitis A Systematic Review of Diagnosis and TreatmentDocument18 pagesConjunctivitis A Systematic Review of Diagnosis and TreatmentdasityarachmanNo ratings yet
- Instilling Otic/Ear Drops Procedure RationaleDocument12 pagesInstilling Otic/Ear Drops Procedure RationaleBSN2-F MASINING NA PAGPAPAHAYAGNo ratings yet
- Pulpotomy Pediatric Prevention Diagnosis Treatment PlanningDocument122 pagesPulpotomy Pediatric Prevention Diagnosis Treatment PlanningTamara Nitya ArianiNo ratings yet
- Antibiotic Decision Making in IcuDocument11 pagesAntibiotic Decision Making in IcumalvindersahiNo ratings yet
- Introduction To The Immune System: Department of Biotechnology Ramaiah University of Applied Sciences BangaloreDocument86 pagesIntroduction To The Immune System: Department of Biotechnology Ramaiah University of Applied Sciences Bangaloreprathyoosha baskaran100% (1)
- Acid-Base Balance: Graciela Lou F. Mana-Ay, RN, ManDocument68 pagesAcid-Base Balance: Graciela Lou F. Mana-Ay, RN, ManKeshia Joyce LimNo ratings yet
- Double Stimulations During The Follicular and Luteal Phases of Poor Responders in IVF/ICSI Programmes (Shanghai Protocol)Document8 pagesDouble Stimulations During The Follicular and Luteal Phases of Poor Responders in IVF/ICSI Programmes (Shanghai Protocol)Nirmal KumawatNo ratings yet
- A Review of Selected Systemic Antifungal Drugs For Use in Dogs and CatsDocument2 pagesA Review of Selected Systemic Antifungal Drugs For Use in Dogs and CatsannygiacoNo ratings yet