You might also like
- Presents A Free Report:: Cortices: Tapping Into The Untapped Potential of The MindDocument13 pagesPresents A Free Report:: Cortices: Tapping Into The Untapped Potential of The MindjakilaNo ratings yet
- Bodytalk Cortices TechniqueDocument2 pagesBodytalk Cortices Techniqueseledit100% (1)
- SE BodyTalkDocument6 pagesSE BodyTalkajp1000No ratings yet
- Access Student NotesDocument34 pagesAccess Student Notesmartinpacenza32No ratings yet
- BodytalkDocument15 pagesBodytalkEyal HasidNo ratings yet
- Living Tree Orchid Essences HomepageDocument110 pagesLiving Tree Orchid Essences HomepageMaricuelina Omega Tres100% (1)
- The Quantum DynamicDocument8 pagesThe Quantum DynamicDestriNo ratings yet
- Psychological Kinesiology: Changing The Body's Beliefs: WhisenantDocument14 pagesPsychological Kinesiology: Changing The Body's Beliefs: WhisenantRukaphuongNo ratings yet
- Self FlowDocument15 pagesSelf FlowariNo ratings yet
- The Evolution of The Amygdala: Basic FunctionDocument8 pagesThe Evolution of The Amygdala: Basic FunctionJamesComeyJustaBitchNo ratings yet
- Tapping Three BrainsDocument4 pagesTapping Three BrainsSodfa EttafakshiNo ratings yet
- ChakrasDocument2 pagesChakras8022100% (2)
- How Energy Travels in The BodyDocument5 pagesHow Energy Travels in The BodyAravindan Muthu100% (1)
- August 2011 Level 2 Workshop-KKDocument357 pagesAugust 2011 Level 2 Workshop-KKianwhite8438No ratings yet
- Entrainement and The Cranial Rythmic ImpulseDocument7 pagesEntrainement and The Cranial Rythmic ImpulseDenise Mathre100% (1)
- BodyTalk: Exploring the 3 BrainsDocument31 pagesBodyTalk: Exploring the 3 BrainsPenelopeReyesNo ratings yet
- Bodytalk Distant Healing StudyDocument2 pagesBodytalk Distant Healing StudyPenelopeReyesNo ratings yet
- ARK - Meridian Focused TherapyDocument29 pagesARK - Meridian Focused TherapySébastien Van100% (1)
- BodyTalk - One Minute Healing PDFDocument4 pagesBodyTalk - One Minute Healing PDFrupjyotisarmah100% (1)
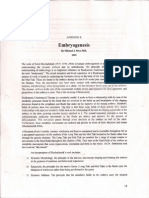
- Embryogenesis SheaDocument4 pagesEmbryogenesis Sheaimageorge13100% (1)
- Jin Shin Jyutsu 1Document3 pagesJin Shin Jyutsu 1virendhemre86% (7)
- Applied Kinesiology: Muscle TestingDocument14 pagesApplied Kinesiology: Muscle TestingLyudmila Danova100% (3)
- Muscle TestingDocument4 pagesMuscle TestingDaniela Stranieri100% (7)
- What Is The Connection Between Chakras and Emotions - The Mood CardsDocument5 pagesWhat Is The Connection Between Chakras and Emotions - The Mood CardsTechnic SelvaNo ratings yet
- Paired MeridiansDocument19 pagesPaired Meridianstibi latis100% (2)
- IAK Kon 2002 Tobar enDocument9 pagesIAK Kon 2002 Tobar enlenuta99No ratings yet
- 5-Phase and Extraordinary Vessels NewDocument9 pages5-Phase and Extraordinary Vessels NewElizabeth Durkee NeilNo ratings yet
- Full Length Talk Transcripts: Enjoy These 3 Expert Talk Transcripts From The Chronic Inflammation Summit!Document52 pagesFull Length Talk Transcripts: Enjoy These 3 Expert Talk Transcripts From The Chronic Inflammation Summit!Antonella DiSatanaNo ratings yet
- Ltoe Chakras ChartDocument1 pageLtoe Chakras ChartAnonymous eLp4uLpOR100% (1)
- Dr. Elisa Rossi Hyperactive Children and Chinese MedicineDocument25 pagesDr. Elisa Rossi Hyperactive Children and Chinese MedicineMichalina Marta MarciniakNo ratings yet
- Muscles & Meridians ChartDocument1 pageMuscles & Meridians ChartilnorisNo ratings yet
- As Above So Below AcupunctureDocument5 pagesAs Above So Below AcupunctureDarren StarwynnNo ratings yet
- Neurovascular Holding PointsDocument8 pagesNeurovascular Holding PointsAlexandru Baciu100% (1)
- BodyTalk Case Studies BookletDocument42 pagesBodyTalk Case Studies BookletAntonella Ercolani100% (2)
- Bladder Meridian - Guardian of PeaceDocument7 pagesBladder Meridian - Guardian of Peacemanket59No ratings yet
- Art Martin and Janes Landrell - Neuro KinesiologyDocument91 pagesArt Martin and Janes Landrell - Neuro KinesiologySharon Anyosa Medina100% (2)
- Tapas WorkbookDocument10 pagesTapas WorkbookWei Bin Thye100% (1)
- Sympathetic Reactivity During Meditation Joan H Hageman (Vol 19 No 2)Document26 pagesSympathetic Reactivity During Meditation Joan H Hageman (Vol 19 No 2)Cambiador de MundoNo ratings yet
- 2013 Perth 3 Course - GuideDocument38 pages2013 Perth 3 Course - GuideDori BarreirosNo ratings yet
- GW Hardin - How To Create Harmonetic WaterDocument2 pagesGW Hardin - How To Create Harmonetic WaterKennethZhangNo ratings yet
- Basic Grid BookletDocument12 pagesBasic Grid BookletSue Martin100% (5)
- NK Course Guide enDocument52 pagesNK Course Guide enIgnacioNo ratings yet
- Eyebody IntroductionDocument15 pagesEyebody Introductionozis6983No ratings yet
- Energy Testing YourselfDocument30 pagesEnergy Testing Yourselfsale18100% (4)
- J S J - Project Summary Sheet: IN HIN YutsuDocument2 pagesJ S J - Project Summary Sheet: IN HIN YutsuFitriandina NitaNo ratings yet
- Touch For Health Casework02-Amy Choi Eng 2019Document15 pagesTouch For Health Casework02-Amy Choi Eng 2019RukaphuongNo ratings yet
- Healing Report ChiDocument81 pagesHealing Report ChiXana Gonçalves100% (1)
- Climbing Elven Stairways DNA As A Macroscopic Metaphor of Polarized PsychodynamicsDocument59 pagesClimbing Elven Stairways DNA As A Macroscopic Metaphor of Polarized PsychodynamicsThiện HoàngNo ratings yet
- Hal 578 SD 586 - Deenadearlova Putri Daryani - EnglishDocument9 pagesHal 578 SD 586 - Deenadearlova Putri Daryani - EnglishDeenadearlova Putri DaryaniNo ratings yet
- Triple Warmer Meridian Acu-Points ChartDocument1 pageTriple Warmer Meridian Acu-Points ChartVicaas VSNo ratings yet
- Words That Touch: How To Ask Questions Your Body Can Answer - 12 Essential 'Clean Questions' For Mind/Body Therapists - PsychotherapyDocument4 pagesWords That Touch: How To Ask Questions Your Body Can Answer - 12 Essential 'Clean Questions' For Mind/Body Therapists - PsychotherapyjunijyjoNo ratings yet
- The Physiology of Muscle MonitoringDocument12 pagesThe Physiology of Muscle MonitoringJalil CabañasNo ratings yet
- Spiritual Portraits of the Energy Release PointsFrom EverandSpiritual Portraits of the Energy Release PointsRating: 5 out of 5 stars5/5 (1)
- Spiritual Healing in Hospitals and Clinics: Scientific Evidence that Energy Medicine Promotes Speedy Recovery and Positive OutcomesFrom EverandSpiritual Healing in Hospitals and Clinics: Scientific Evidence that Energy Medicine Promotes Speedy Recovery and Positive OutcomesRating: 1 out of 5 stars1/5 (1)
- Cre Final PDFDocument147 pagesCre Final PDFGeeta Rameshsingh ThakurNo ratings yet
- Peer Pressure and FOMO: Causes, Effects and How to OvercomeDocument5 pagesPeer Pressure and FOMO: Causes, Effects and How to OvercomeAaryan ChhabraNo ratings yet
- Culture and PsychopathologyDocument7 pagesCulture and PsychopathologyKrishan TewatiaNo ratings yet
- Social Work Stress BurnoutDocument12 pagesSocial Work Stress BurnoutCooky GreeceNo ratings yet
- Atlas of Operative Maxillofacial Trauma Surgery - Michael Perry (2020)Document940 pagesAtlas of Operative Maxillofacial Trauma Surgery - Michael Perry (2020)doc.khudykNo ratings yet
- H.O.P.E. 2 Module 1Document23 pagesH.O.P.E. 2 Module 1Reynaldo Jr LundagNo ratings yet
- Anxiety Ignorance A Psychological Study of Developmental Step of Growing Up Described in Peterpan Movie (2003)Document146 pagesAnxiety Ignorance A Psychological Study of Developmental Step of Growing Up Described in Peterpan Movie (2003)Hamka khamidahNo ratings yet
- Addressing student council's art festival planDocument10 pagesAddressing student council's art festival planWeviNo ratings yet
- Rothblum, Solomon, Murakami 1986 - Diferencias Cognitivas, Afectivas y Conductuales Entre Procrastinadores Altos y BajosDocument8 pagesRothblum, Solomon, Murakami 1986 - Diferencias Cognitivas, Afectivas y Conductuales Entre Procrastinadores Altos y BajosMartin RuízNo ratings yet
- The Brief Symptom Inventory An Introductory ReportDocument5 pagesThe Brief Symptom Inventory An Introductory ReportSubhan AnsariNo ratings yet
- The Brain Disease Model of Addiction: Butler Center For Research May 2021Document2 pagesThe Brain Disease Model of Addiction: Butler Center For Research May 2021cultura84No ratings yet
- S3 Perinatal DeppressionDocument15 pagesS3 Perinatal DeppressionAmir Iqbal Mallick100% (1)
- My Little PonyDocument10 pagesMy Little Ponyapi-565360584No ratings yet
- An Art Therapy Group For ChildrenDocument31 pagesAn Art Therapy Group For Childrenclaudia mihaiNo ratings yet
- Payton Neville Final PaperDocument12 pagesPayton Neville Final Paperapi-549079854No ratings yet
- Sexual Dysfunction in Depression and Anxiety - Conceptualizing Sexual Dysfunction As Part of An Internalizing DimensionDocument13 pagesSexual Dysfunction in Depression and Anxiety - Conceptualizing Sexual Dysfunction As Part of An Internalizing DimensionvickyreyeslucanoNo ratings yet
- Steps To An Ecology of Self Implications For HomeopathyDocument5 pagesSteps To An Ecology of Self Implications For HomeopathyDr Kenneth SilvestriNo ratings yet
- Physical Education and Health 2: BSBT College, IncDocument21 pagesPhysical Education and Health 2: BSBT College, IncDM Camilot IINo ratings yet
- Assessment Overview: Symptom Checklist 90 Revised (SCL-90-R)Document2 pagesAssessment Overview: Symptom Checklist 90 Revised (SCL-90-R)livius bolohanNo ratings yet
- 8 - Sullivan - Interpersonal TheoryDocument11 pages8 - Sullivan - Interpersonal TheoryAuie Trajano100% (1)
- Alzheimers Disease and The Impact of Music TherapyDocument11 pagesAlzheimers Disease and The Impact of Music TherapyJoe Perry100% (1)
- Gender Identity in Informal Care: Impact On Health in Spanish CaregiversDocument15 pagesGender Identity in Informal Care: Impact On Health in Spanish CaregiversAUCANLATINMAILNo ratings yet
- Depression Facts: Causes, Symptoms and TreatmentDocument5 pagesDepression Facts: Causes, Symptoms and TreatmentStargazerNo ratings yet
- 6 Review Article OnychophagiaDocument8 pages6 Review Article OnychophagiaAmalia HusnaNo ratings yet
- Guide To Tackling Maths Anxiety Power Maths ReportDocument32 pagesGuide To Tackling Maths Anxiety Power Maths ReportTSGNo ratings yet
- The Mindful Nurse Leader Improving Processes And.11Document4 pagesThe Mindful Nurse Leader Improving Processes And.11Khryss Paula BaldonadoNo ratings yet
- Hypnoanalysis and Analytical Hypnotherapy Vol3Document255 pagesHypnoanalysis and Analytical Hypnotherapy Vol3brice lemaireNo ratings yet
- 1983 - The Brief Symptom Inventory, An Introductory ReportDocument11 pages1983 - The Brief Symptom Inventory, An Introductory ReportBogdan BaceanuNo ratings yet
- Sample LTR - Extreme HardshipDocument3 pagesSample LTR - Extreme HardshipCarlosNo ratings yet
- The Inferiority Complex Cure - The Ultimate Guide To Raise Your Self-Esteem and Overcome Your Inferiority ComplexDocument36 pagesThe Inferiority Complex Cure - The Ultimate Guide To Raise Your Self-Esteem and Overcome Your Inferiority ComplexAretha Dawes100% (1)