You might also like
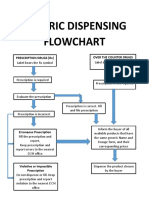
- Generic Dispensing Flowchart: Over The Counter Drugs Prescription Drugs (RX)Document1 pageGeneric Dispensing Flowchart: Over The Counter Drugs Prescription Drugs (RX)chibibi the gr67% (3)
- Risk Management PlanDocument2 pagesRisk Management PlanKeith Reyes100% (3)
- Generic Dispensing Flowchart: Over The Counter Drugs Prescription Drugs (RX)Document1 pageGeneric Dispensing Flowchart: Over The Counter Drugs Prescription Drugs (RX)chibibi the grNo ratings yet
- AO 56 S 1989 LTODocument13 pagesAO 56 S 1989 LTOmikan2No ratings yet
- RMP For Drug Establishments - 26 August 2015 PDFDocument88 pagesRMP For Drug Establishments - 26 August 2015 PDFIan FranklinNo ratings yet
- ADR Form PDFDocument1 pageADR Form PDFChatie PipitNo ratings yet
- GMC Kathua SOP for Pharmacy and Stores ManagementDocument25 pagesGMC Kathua SOP for Pharmacy and Stores ManagementSauraj GautamNo ratings yet
- Generic Menu CardDocument13 pagesGeneric Menu CardCarissa Villaver100% (2)
- RMP For Drug Establishments - 26 August 2015 PDFDocument88 pagesRMP For Drug Establishments - 26 August 2015 PDFBelle BrionesNo ratings yet
- DTLNHS Pharmacy SOPDocument5 pagesDTLNHS Pharmacy SOPCindy Gabayeron100% (1)
- For External Use Only For External Use OnlyDocument1 pageFor External Use Only For External Use OnlyRacel BandongNo ratings yet
- Standard Operating Procedure 4 PDF FreeDocument19 pagesStandard Operating Procedure 4 PDF FreeMillen100% (2)
- Unit 1. Clinical PharmacyDocument5 pagesUnit 1. Clinical PharmacyAashish BhattaraiNo ratings yet
- FDH Pharmacy Risk Management PlanDocument7 pagesFDH Pharmacy Risk Management PlanLexie GleeNo ratings yet
- Module 1-Introduction To Health Technology AssessmentDocument3 pagesModule 1-Introduction To Health Technology AssessmentLou Calderon100% (1)
- Personnel Competency EvaluationDocument4 pagesPersonnel Competency EvaluationMikes Flores100% (1)
- Pharmacist Duties: Prepare Medications, Counsel PatientsDocument3 pagesPharmacist Duties: Prepare Medications, Counsel Patientsisabel agredaNo ratings yet
- Standard Operating Procedure Good Dispensing PracticeDocument2 pagesStandard Operating Procedure Good Dispensing PracticeDaniel Yves IV Paez100% (1)
- Edpms Complete GuideDocument75 pagesEdpms Complete Guidesheryl GuillermoNo ratings yet
- Transfer of Medicines SOPDocument3 pagesTransfer of Medicines SOPPROBLEMSOLVERNo ratings yet
- Pharmaceutical Dosage Forms GuideDocument62 pagesPharmaceutical Dosage Forms GuideYsmael MagnoNo ratings yet
- Standard Patient Counseling ScriptDocument22 pagesStandard Patient Counseling ScriptElleason Joshua G. FranciscoNo ratings yet
- DispensingDocument30 pagesDispensingNamanamanaNo ratings yet
- Role and Responsibility of Pharmacy Assistant in Community PharmacyDocument4 pagesRole and Responsibility of Pharmacy Assistant in Community PharmacyUntouchable Monster 2No ratings yet
- Generic drug dispensing process flowDocument1 pageGeneric drug dispensing process flowBUPHARCO Mintal Branch100% (1)
- Standard Operating Procedure Good Storage PracticeDocument2 pagesStandard Operating Procedure Good Storage PracticeDaniel Yves IV Paez100% (1)
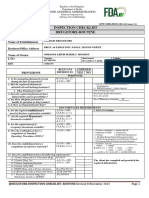
- FDA Inspection Checklist for Sardam Drugstore RoutineDocument3 pagesFDA Inspection Checklist for Sardam Drugstore RoutineJohanna MonroyNo ratings yet
- Internship 1 therapeutic categories PNDFDocument75 pagesInternship 1 therapeutic categories PNDFMariah Sharmane Juego Santos100% (2)
- CAPA Plan Farmacia Delim and General MerchandiseDocument4 pagesCAPA Plan Farmacia Delim and General MerchandiseArianne Courtney Nacar100% (1)
- PHARMACY AND THERAPEUTICS COMMITTEE Edited 12345Document38 pagesPHARMACY AND THERAPEUTICS COMMITTEE Edited 12345Shafaqat Ghani Shafaqat Ghani100% (3)
- Patient SafetyDocument105 pagesPatient SafetyAre Pee EtcNo ratings yet
- Activity 11 19Document23 pagesActivity 11 19RyannDeLeonNo ratings yet
- Generic Menu CardDocument9 pagesGeneric Menu CardLode DeocadesNo ratings yet
- Chapter 5 Hospital FormularyDocument6 pagesChapter 5 Hospital Formularyiamgerardgarces100% (15)
- Hospital Pharmacy Activity ManualDocument30 pagesHospital Pharmacy Activity ManualNathaniel BarratoNo ratings yet
- IEC-60721-3-3-2019 (Enviromental Conditions)Document12 pagesIEC-60721-3-3-2019 (Enviromental Conditions)Electrical DistributionNo ratings yet
- Oracle Fusion Financials Book Set Home Page SummaryDocument274 pagesOracle Fusion Financials Book Set Home Page SummaryAbhishek Agrawal100% (1)
- Little Book of Effective WritingDocument44 pagesLittle Book of Effective Writingshalashvili100% (1)
- Requirements For Opening A Drugstore PDFDocument2 pagesRequirements For Opening A Drugstore PDFPsyar Lysa Javier100% (2)
- Damasco - Cpi - Activity No.9Document5 pagesDamasco - Cpi - Activity No.9LDCU - Damasco, Erge Iris M.No ratings yet
- Mba Project GuidelinesDocument8 pagesMba Project GuidelinesKrishnamohan VaddadiNo ratings yet
- Ghid Dislipidemie 2019Document78 pagesGhid Dislipidemie 2019Ema PetrescuNo ratings yet
- Ghid Dislipidemie 2019Document78 pagesGhid Dislipidemie 2019Ema PetrescuNo ratings yet
- ADR FormDocument1 pageADR Formultimate_2226252No ratings yet
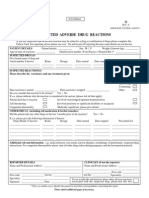
- Suspected Adverse Reaction FormDocument2 pagesSuspected Adverse Reaction FormJonathan Deguzman100% (1)
- Internship5 12Document7 pagesInternship5 12Jerel MarquezNo ratings yet
- Railway PharmasistDocument2 pagesRailway PharmasistprashantNo ratings yet
- Exercises 8-10 (By Dr. N. Tubon) PDFDocument25 pagesExercises 8-10 (By Dr. N. Tubon) PDFLoren100% (1)
- Damasco - Cpi - Activity No. 10Document18 pagesDamasco - Cpi - Activity No. 10LDCU - Damasco, Erge Iris M.No ratings yet
- Ethical Standards for Health Product PromotionDocument14 pagesEthical Standards for Health Product PromotionKitkat CasacopNo ratings yet
- Nica Chua - Hospital Pharmacy Internship Daily Activity Report-Day 33 MajorDocument5 pagesNica Chua - Hospital Pharmacy Internship Daily Activity Report-Day 33 MajorMa Victoria ChuaNo ratings yet
- INTERN-3 Community Pharmacy ProfileDocument34 pagesINTERN-3 Community Pharmacy ProfilejadeNo ratings yet
- Ppgp-Mfg-Oc G3 - Pd-2 - CP, CPP, Cqa NOTES On The ActivityDocument5 pagesPpgp-Mfg-Oc G3 - Pd-2 - CP, CPP, Cqa NOTES On The ActivityIsabel Peralta50% (2)
- Cpi - Damasco - Activity 25 & 26Document3 pagesCpi - Damasco - Activity 25 & 26LDCU - Damasco, Erge Iris M.No ratings yet
- ADR Reporting of Rash from AntibioticDocument4 pagesADR Reporting of Rash from AntibioticJonathan DeguzmanNo ratings yet
- Advocacy in PharmacyDocument3 pagesAdvocacy in PharmacyZofia RanadaNo ratings yet
- Laws Governing The Community Pharmacy PracticeDocument3 pagesLaws Governing The Community Pharmacy Practicecorreen mendozaNo ratings yet
- PH-PHR212 Lecture 2 FS2021 PDFDocument57 pagesPH-PHR212 Lecture 2 FS2021 PDFIra MoranteNo ratings yet
- Dispensing CA NotesDocument16 pagesDispensing CA NotesJohn TecsonNo ratings yet
- Case 4 - MCNP - Miguel, Mark Darren, T.Document3 pagesCase 4 - MCNP - Miguel, Mark Darren, T.markNo ratings yet
- DRAP New Suspected Adverse Reaction Reporting Form For Health Care Professionals PDFDocument3 pagesDRAP New Suspected Adverse Reaction Reporting Form For Health Care Professionals PDFShakil Khan100% (1)
- Adr Form 10Document3 pagesAdr Form 10doctor uroosaNo ratings yet
- Adr FormDocument2 pagesAdr FormZaira Clarisse de GuzmanNo ratings yet
- Report of Suspected Adverse Drug Reactions: It's Easy To Report Online: Mhra - Gov.uk/yellowcard or Via The AppDocument2 pagesReport of Suspected Adverse Drug Reactions: It's Easy To Report Online: Mhra - Gov.uk/yellowcard or Via The AppGeorgia KavakopoulouNo ratings yet
- Case 3 - MCNP - Miguel, Mark Darren, T.Document3 pagesCase 3 - MCNP - Miguel, Mark Darren, T.markNo ratings yet
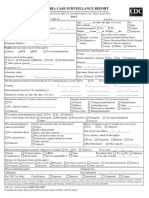
- Malaria Case Surveillance Report SummaryDocument2 pagesMalaria Case Surveillance Report SummaryPramod gameNo ratings yet
- Suspected Adverse Drug Reactions: in ConfidenceDocument1 pageSuspected Adverse Drug Reactions: in ConfidenceSujith KuttanNo ratings yet
- FDA Advisory No.2020 1811 ADocument2 pagesFDA Advisory No.2020 1811 AAre Pee EtcNo ratings yet
- FDA Advisory No.2021 2470Document2 pagesFDA Advisory No.2021 2470Are Pee EtcNo ratings yet
- Americanchesscod00brit PDFDocument76 pagesAmericanchesscod00brit PDFIscNo ratings yet
- Reasons To Be A PharTechDocument1 pageReasons To Be A PharTechAre Pee EtcNo ratings yet
- Chess Review 1933 - 1Document36 pagesChess Review 1933 - 1Are Pee EtcNo ratings yet
- ACC-AHA Lipid Guidelines - Personalized Care To Prevent Cardiovascular DiseaseDocument9 pagesACC-AHA Lipid Guidelines - Personalized Care To Prevent Cardiovascular DiseaseAre Pee EtcNo ratings yet
- Chess Review 1933 - 1Document36 pagesChess Review 1933 - 1Are Pee EtcNo ratings yet
- Medication Errors - Where Do They Happen - The Pharmaceutical JournalDocument7 pagesMedication Errors - Where Do They Happen - The Pharmaceutical JournalAre Pee EtcNo ratings yet
- ASHP Guidelines On Managing Drug Product Shortages: PurposeDocument9 pagesASHP Guidelines On Managing Drug Product Shortages: PurposeAsma Al-MahmoudNo ratings yet
- Americanchesscod00brit PDFDocument76 pagesAmericanchesscod00brit PDFIscNo ratings yet
- Use Medicines WiselyDocument1 pageUse Medicines WiselyAre Pee EtcNo ratings yet
- Americanchesscod00brit PDFDocument76 pagesAmericanchesscod00brit PDFIscNo ratings yet
- Achieving Healthy Weight Final 0 0Document1 pageAchieving Healthy Weight Final 0 0Are Pee EtcNo ratings yet
- Heart Healthy Eating Dash Style Final 1 0Document1 pageHeart Healthy Eating Dash Style Final 1 0Are Pee EtcNo ratings yet
- Guidelines Managaement of Blood CholesterolDocument36 pagesGuidelines Managaement of Blood CholesterolAre Pee EtcNo ratings yet
- Tips For Eating Heart-Healthy South Asian StyleDocument1 pageTips For Eating Heart-Healthy South Asian StyleAre Pee EtcNo ratings yet
- Achieving Healthy Weight Final 0 0Document1 pageAchieving Healthy Weight Final 0 0Are Pee EtcNo ratings yet
- PH Tax RMC No 19 2015 NoexpDocument1 pagePH Tax RMC No 19 2015 NoexpRodel Ryan YanaNo ratings yet
- Legal Basis of Health Education in The Philippines - PicsHealthDocument13 pagesLegal Basis of Health Education in The Philippines - PicsHealthAre Pee EtcNo ratings yet
- Tax Guide For Professionals BIRDocument8 pagesTax Guide For Professionals BIRPY CaunanNo ratings yet
- For Your Free, Tailored, Daily Legal Newsfeed ServiceDocument9 pagesFor Your Free, Tailored, Daily Legal Newsfeed ServiceAre Pee EtcNo ratings yet
- Income Tax - Bureau of Internal RevenueDocument21 pagesIncome Tax - Bureau of Internal RevenueAre Pee EtcNo ratings yet
- Legal Basis of Health Education in The Philippines - PicsHealthDocument13 pagesLegal Basis of Health Education in The Philippines - PicsHealthAre Pee EtcNo ratings yet
- For Your Free, Tailored, Daily Legal Newsfeed ServiceDocument9 pagesFor Your Free, Tailored, Daily Legal Newsfeed ServiceAre Pee EtcNo ratings yet
- Garbage Recycling InfographicsDocument1 pageGarbage Recycling InfographicsAre Pee EtcNo ratings yet
- RA 10586 - Anti-Drunk and Drugged Driving Act of 2013Document2 pagesRA 10586 - Anti-Drunk and Drugged Driving Act of 2013Are Pee EtcNo ratings yet
- For Your Free, Tailored, Daily Legal Newsfeed ServiceDocument9 pagesFor Your Free, Tailored, Daily Legal Newsfeed ServiceAre Pee EtcNo ratings yet
- Credit Risk Management Practice in Private Banks Case Study Bank of AbyssiniaDocument85 pagesCredit Risk Management Practice in Private Banks Case Study Bank of AbyssiniaamogneNo ratings yet
- 4 - Complex IntegralsDocument89 pages4 - Complex IntegralsryuzackyNo ratings yet
- Test SessionDocument2 pagesTest SessionMuhammad Fiaz AslamNo ratings yet
- WA Beretta M92FS Parts ListDocument2 pagesWA Beretta M92FS Parts ListDenis Deki NehezNo ratings yet
- Application Programming InterfaceDocument12 pagesApplication Programming InterfacesorinproiecteNo ratings yet
- EG-45-105 Material Information Sheet (Textura) V2Document4 pagesEG-45-105 Material Information Sheet (Textura) V2GPRNo ratings yet
- AIATS 2021 (OYMCF) Test 01 Offline - Code A - SolutionsDocument34 pagesAIATS 2021 (OYMCF) Test 01 Offline - Code A - Solutionsbhavyakavya mehta100% (1)
- Zhihua Yao - Dignaga and The 4 Types of Perception (JIP 04)Document24 pagesZhihua Yao - Dignaga and The 4 Types of Perception (JIP 04)Carlos Caicedo-Russi100% (1)
- Technical File D13-MH, MG IMO Tier 11 GLDocument18 pagesTechnical File D13-MH, MG IMO Tier 11 GLsfsdffdsdfsdfsdfNo ratings yet
- Startups Helping - India Go GreenDocument13 pagesStartups Helping - India Go Greensimran kNo ratings yet
- Docking 1Document12 pagesDocking 1Naveen Virendra SinghNo ratings yet
- Assessing Eyes NCM 103 ChecklistDocument7 pagesAssessing Eyes NCM 103 ChecklistNicole NipasNo ratings yet
- Phys114 Ps 1Document11 pagesPhys114 Ps 1Reine Amabel JarudaNo ratings yet
- EQ - Module - Cantilever MethodDocument17 pagesEQ - Module - Cantilever MethodAndrea MalateNo ratings yet
- Vintage Style Indonesian Geography Lesson For High School by SlidesgoDocument56 pagesVintage Style Indonesian Geography Lesson For High School by Slidesgoohd InstalasicontrolNo ratings yet
- Product Catalog 2016Document84 pagesProduct Catalog 2016Sauro GordiniNo ratings yet
- Body Scan AnalysisDocument9 pagesBody Scan AnalysisAmaury CosmeNo ratings yet
- ASD Manual and AISC LRFD Manual For Bolt Diameters Up To 6 Inches (150Document1 pageASD Manual and AISC LRFD Manual For Bolt Diameters Up To 6 Inches (150rabzihNo ratings yet
- SuffrageDocument21 pagesSuffragejecelyn mae BaluroNo ratings yet
- 277Document18 pages277Rosy Andrea NicolasNo ratings yet
- Biomechanics of Advanced Tennis: January 2003Document7 pagesBiomechanics of Advanced Tennis: January 2003Katrien BalNo ratings yet
- Chapter 9-10 (PPE) Reinzo GallegoDocument48 pagesChapter 9-10 (PPE) Reinzo GallegoReinzo GallegoNo ratings yet
- April 3rd - Asynchronous Class - Questions-4Document3 pagesApril 3rd - Asynchronous Class - Questions-4alidrissiNo ratings yet
- Plant Air Centrifugal Compressors: Turbo-Air Series Featuring Oil-Free AirDocument20 pagesPlant Air Centrifugal Compressors: Turbo-Air Series Featuring Oil-Free AirSharad KokateNo ratings yet
- Summer Internship Project-NishantDocument80 pagesSummer Internship Project-Nishantnishant singhNo ratings yet
- Manual Bombas CHWDocument16 pagesManual Bombas CHWFred GarciaNo ratings yet