You might also like
- Agile Outcome Measures Ems v2Document8 pagesAgile Outcome Measures Ems v2Ndruew FujiwaraNo ratings yet
- Agile Outcome Measures Ems v2Document2 pagesAgile Outcome Measures Ems v2Aaliyah ShaikhNo ratings yet
- Guidelines for Falls Risk AssessmentDocument2 pagesGuidelines for Falls Risk AssessmentAnonymous tbJ24554No ratings yet
- You Can Study Starred Terms Together: Star This TermDocument25 pagesYou Can Study Starred Terms Together: Star This TermAnAs Al ArjanNo ratings yet
- How Often Should Sitting and Rising From A Chair Be Evaluated in Patients With Duchenne Muscular Dystrophy?Document6 pagesHow Often Should Sitting and Rising From A Chair Be Evaluated in Patients With Duchenne Muscular Dystrophy?JoNo ratings yet
- Functional AssessmentDocument52 pagesFunctional AssessmentCelina Tam Ching LamNo ratings yet
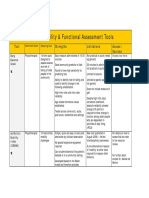
- Assessment Tools for Mobility & Functional IndependenceDocument4 pagesAssessment Tools for Mobility & Functional Independencesonya63265No ratings yet
- The Concurrent Validity and Reliability of The Leg Motion System For Measuring Ankle Dorsiflexion Range of Motion in Older AdultsDocument14 pagesThe Concurrent Validity and Reliability of The Leg Motion System For Measuring Ankle Dorsiflexion Range of Motion in Older AdultsFacu YaneNo ratings yet
- Mobility AssestmentDocument3 pagesMobility Assestmentfrancisco.quispemedinaNo ratings yet
- The Timed Up & Go - A Test of Basic Functional Mobility For Frail Elderly Persons. lAGSDocument7 pagesThe Timed Up & Go - A Test of Basic Functional Mobility For Frail Elderly Persons. lAGSJose Fernando Díez ConchaNo ratings yet
- Katz Index of Independence in Activities of Daily LivingDocument5 pagesKatz Index of Independence in Activities of Daily LivingDick Morgan FerrerNo ratings yet
- Assessing Functional AbilityDocument15 pagesAssessing Functional AbilitySonali Soumyashree100% (2)
- Wisci GuideDocument4 pagesWisci GuideJosé Alfonso Batún MayNo ratings yet
- Balance Assessment HandbookDocument18 pagesBalance Assessment Handbookjega_physioNo ratings yet
- Outcome Measures - NeuroDocument28 pagesOutcome Measures - NeurorthathapNo ratings yet
- Functional Reach Arm Test (FRT)Document7 pagesFunctional Reach Arm Test (FRT)AnisDwiUlfahndariNo ratings yet
- Lab2 HowfitareyouDocument6 pagesLab2 Howfitareyouapi-500185788No ratings yet
- College Nursing Ambulation CaneDocument2 pagesCollege Nursing Ambulation CaneMac Cristian A. CaraganNo ratings yet
- Measurement and Scales Used in PhysiotherapyDocument38 pagesMeasurement and Scales Used in PhysiotherapyAnurag BhuyanNo ratings yet
- Ali Taki Neutral PostureDocument16 pagesAli Taki Neutral PostureMohammad DashtiNo ratings yet
- Comparison of mini-bestest and dynamic gait index for prediction of fall susceptibility in old individualsDocument5 pagesComparison of mini-bestest and dynamic gait index for prediction of fall susceptibility in old individualsElahe SadeqiNo ratings yet
- Module 4 Functional AssessmentDocument12 pagesModule 4 Functional AssessmentStephanie DilloNo ratings yet
- Clinical Resource PacketDocument3 pagesClinical Resource Packetoscar alvaradoNo ratings yet
- Ambulation: The Ability To Move From Place To Place With or Without Assistive DeviceDocument41 pagesAmbulation: The Ability To Move From Place To Place With or Without Assistive DeviceGrape JuiceNo ratings yet
- AmbulationetcDocument41 pagesAmbulationetcNathaniel Karl Enin PulidoNo ratings yet
- Assessment of The Test-Retest Reliability and Construct Validity of A Modified Lequesne Index in Knee OsteoarthritisDocument6 pagesAssessment of The Test-Retest Reliability and Construct Validity of A Modified Lequesne Index in Knee OsteoarthritisKanliajie Kresna KastiantoNo ratings yet
- UW Health Job for Endoscopy TechnicianDocument2 pagesUW Health Job for Endoscopy TechnicianAnupam KumarNo ratings yet
- 2017 Article 1388Document10 pages2017 Article 1388MonikaNo ratings yet
- R.N Ohood F. ShunnarDocument50 pagesR.N Ohood F. ShunnarOhood ShunnarNo ratings yet
- Myelomeningocele classificationDocument5 pagesMyelomeningocele classificationLema Ulloa ZoraidaNo ratings yet
- BMAT-Bedside Mobility Assessment Tool: by Amber Perez ADN, BSB, CSPHPDocument36 pagesBMAT-Bedside Mobility Assessment Tool: by Amber Perez ADN, BSB, CSPHPConvalescent Nursing HomeNo ratings yet
- AlphaFIM - HelpFul - Hints 2Document12 pagesAlphaFIM - HelpFul - Hints 2Ciaren FonsecaNo ratings yet
- Geriatric AssessmentDocument28 pagesGeriatric AssessmentSanjanaa ZadNo ratings yet
- Health AssessmentDocument23 pagesHealth AssessmentPORTRAIT OF A NURSENo ratings yet
- Realosa PresentationDocument14 pagesRealosa PresentationSharalyn SiaNo ratings yet
- PR 2Document6 pagesPR 2Andrei ArtiedaNo ratings yet
- 2013 Table 1 Mobility and Functional Assessment Tools PDFDocument4 pages2013 Table 1 Mobility and Functional Assessment Tools PDFesbat07No ratings yet
- Prioritizing Elderly Comfort for Effective Geriatric AssessmentDocument2 pagesPrioritizing Elderly Comfort for Effective Geriatric AssessmentJona Joyce JunsayNo ratings yet
- Assignment On Video Display Worksation: Submited byDocument21 pagesAssignment On Video Display Worksation: Submited byKhayrulIslamNo ratings yet
- Discussion Forum PDDocument3 pagesDiscussion Forum PDMark Angelo CañeteNo ratings yet
- Health & Safety Guide: HSG0509 Fitness and Aptitude Assessment Guidelines For Working in Confined SpacesDocument13 pagesHealth & Safety Guide: HSG0509 Fitness and Aptitude Assessment Guidelines For Working in Confined SpacesRuggiero Fernandez MarianellaNo ratings yet
- 2 Minute Walk TestDocument10 pages2 Minute Walk TestTomer NobelNo ratings yet
- Functional Status Score For The Intensive Care Unit (FSS-ICU) General Guidelines For ScoringDocument7 pagesFunctional Status Score For The Intensive Care Unit (FSS-ICU) General Guidelines For ScoringBennisonNo ratings yet
- Nursing Musculoskeletal Physical AssessmentDocument14 pagesNursing Musculoskeletal Physical AssessmentilhamNo ratings yet
- Responsiveness of The Mini-Bestest and Berg Comparison of Reliability, Validity, andDocument12 pagesResponsiveness of The Mini-Bestest and Berg Comparison of Reliability, Validity, andRidho RizkianandaNo ratings yet
- Understanding Visual Fields Part I Goldmann PerimeDocument11 pagesUnderstanding Visual Fields Part I Goldmann PerimeAngelaNo ratings yet
- Ims 1 10 18Document2 pagesIms 1 10 18Katherine UrregoNo ratings yet
- Elderly Mobility Scale-Letter (2016) 2Document2 pagesElderly Mobility Scale-Letter (2016) 2Celina Tam Ching LamNo ratings yet
- FLEXIBILITY AND AGILITY CORRELATION IN ATHLETESDocument4 pagesFLEXIBILITY AND AGILITY CORRELATION IN ATHLETESShivam RavalNo ratings yet
- 2017 - Menezes Et Al. - Instruments To Evaluate Mobility CapacityDocument13 pages2017 - Menezes Et Al. - Instruments To Evaluate Mobility CapacityMaria Paula Bastos DiasNo ratings yet
- Pi Is 0161642012009815Document7 pagesPi Is 0161642012009815Qonita WachidahNo ratings yet
- 5 PASAY PE11 S1 Q1 W3 EditedDocument3 pages5 PASAY PE11 S1 Q1 W3 EditedJaeNo ratings yet
- Owas MethodDocument22 pagesOwas MethodLo Roque100% (2)
- Choosing the Correct Walking Aid for PatientsDocument2 pagesChoosing the Correct Walking Aid for PatientsRahmanu ReztaputraNo ratings yet
- Length Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesRating: 3.5 out of 5 stars3.5/5 (3)
- Tests AptaDocument7 pagesTests AptaGiusePpe MeatzaNo ratings yet
- The Role of Occupational Therapy for ALS PatientsDocument27 pagesThe Role of Occupational Therapy for ALS PatientsPa T EthiopiaNo ratings yet
- After Sci EvaluationDocument22 pagesAfter Sci EvaluationManos AndriolasNo ratings yet
- Barthel IndexDocument4 pagesBarthel IndexrlinaoNo ratings yet
- Shoulder TrainingDocument12 pagesShoulder TrainingOscar NgNo ratings yet
- Clinical: ResearchDocument5 pagesClinical: ResearchjusudNo ratings yet
- 61Document8 pages61jusudNo ratings yet
- Ela AmbarwatiDocument8 pagesEla AmbarwatialvinNo ratings yet
- 2 PDFDocument7 pages2 PDFjusudNo ratings yet
- Bookshelf NBK204 PDFDocument3 pagesBookshelf NBK204 PDFjusudNo ratings yet
- Sing KatanDocument1 pageSing KatanjusudNo ratings yet
- Faktor-Faktor Yang Berhubungan Dengan Status Gizi Usila Di Kota Padang Tahun 2006Document4 pagesFaktor-Faktor Yang Berhubungan Dengan Status Gizi Usila Di Kota Padang Tahun 2006jusudNo ratings yet
- Relationship between Serum Albumin and AgingDocument6 pagesRelationship between Serum Albumin and AgingjusudNo ratings yet
- Faktor-Faktor Yang Berhubungan Dengan Status Gizi Usila Di Kota Padang Tahun 2006Document4 pagesFaktor-Faktor Yang Berhubungan Dengan Status Gizi Usila Di Kota Padang Tahun 2006jusudNo ratings yet
- 1989 Modified Barthel IndexDocument7 pages1989 Modified Barthel IndexoriogonNo ratings yet
- Barthel ADLsDocument3 pagesBarthel ADLsGamaliel SeasonNo ratings yet
- Barthel Index (0-20)Document2 pagesBarthel Index (0-20)Yessika Adelwin Natalia95% (19)
- Inter-Rater Reliability of The Original and Modified Barthel Index, and A Comparison With The Functional Independence MeasureDocument8 pagesInter-Rater Reliability of The Original and Modified Barthel Index, and A Comparison With The Functional Independence Measurelolocy LNo ratings yet
- Barthel Index For Stroke Trials Development, Properties, and ApplicationDocument6 pagesBarthel Index For Stroke Trials Development, Properties, and ApplicationDewi HidajatiNo ratings yet
- Barthel Index of Activities of Daily LivDocument2 pagesBarthel Index of Activities of Daily LivFerrari RomanoNo ratings yet
- The Barthel ADL Index: A Reliability Study : Rivermead Rehabilitation Centre, Bingdon Road, Oxford, Great BritainDocument3 pagesThe Barthel ADL Index: A Reliability Study : Rivermead Rehabilitation Centre, Bingdon Road, Oxford, Great BritainLuis Carlos Venegas SanabriaNo ratings yet
- Barthel FIM StrokeDocument5 pagesBarthel FIM StrokemarisolNo ratings yet
- Barthel Index of Activities of Daily Living assessment toolDocument1 pageBarthel Index of Activities of Daily Living assessment toolJU WSDNo ratings yet
- Outcome BarthelDocument5 pagesOutcome BarthelEncep Ivan SetiawanNo ratings yet
- Measures of Adult General Functional Status - The BarthelDocument13 pagesMeasures of Adult General Functional Status - The BarthelLila CoxNo ratings yet
- Home Health ToolboxDocument32 pagesHome Health ToolboxFred TomNo ratings yet
- THE Barthel Index: Patient Name: Rater Name: Date: Keeli Therrien October 26 20Document2 pagesTHE Barthel Index: Patient Name: Rater Name: Date: Keeli Therrien October 26 20AminGinanjarPNo ratings yet
- Barthel Index of Activities of Daily Living Assessment ToolDocument2 pagesBarthel Index of Activities of Daily Living Assessment ToolgarbagepatchNo ratings yet
- Barthel IndexDocument1 pageBarthel IndexChu Ai Reen50% (2)
- Agile Outcome Measures Ems v2 PDFDocument8 pagesAgile Outcome Measures Ems v2 PDFjusudNo ratings yet
- The Timed Up & Go - A Test of Basic Functional Mobility For Frail Elderly Persons. lAGSDocument7 pagesThe Timed Up & Go - A Test of Basic Functional Mobility For Frail Elderly Persons. lAGSJose Fernando Díez ConchaNo ratings yet
- Barthel IndexDocument2 pagesBarthel Indexgania100% (1)
- Leung 2007Document11 pagesLeung 2007leonardo mustopoNo ratings yet
- Barthels Index of ADLs PDFDocument4 pagesBarthels Index of ADLs PDFWindaNo ratings yet
- Barthel IndexDocument4 pagesBarthel IndexrlinaoNo ratings yet
- Evaluation, Tests and Measures in Physical TherapyDocument339 pagesEvaluation, Tests and Measures in Physical TherapywanderlastNo ratings yet
- Activities of Daily Living Scales and Functional Independence MeasureDocument45 pagesActivities of Daily Living Scales and Functional Independence Measurewahyana mujari wahidNo ratings yet
- Barthel Index in The Spanish Population Widely Used But Without 2018Document2 pagesBarthel Index in The Spanish Population Widely Used But Without 2018Umi IstianahNo ratings yet
- Barthels and KatzDocument13 pagesBarthels and KatzrlinaoNo ratings yet
- Barthel IndexDocument4 pagesBarthel IndexSuhana PathanNo ratings yet