You might also like
- Vaginitis EmedicineDocument17 pagesVaginitis EmedicineIndah HaneNo ratings yet
- Gyne - (Section B) PID-STI-1Document45 pagesGyne - (Section B) PID-STI-1Kailash KhatriNo ratings yet
- Acute Cervicitis - UpToDateDocument28 pagesAcute Cervicitis - UpToDatePatriciaNo ratings yet
- Family Planing and Sexually Transmitted DiseasesDocument34 pagesFamily Planing and Sexually Transmitted DiseasesRina KawamuraNo ratings yet
- N00159 South Africa Vulvovaginal Candidiasis SEP2016 Rev000Document2 pagesN00159 South Africa Vulvovaginal Candidiasis SEP2016 Rev000Endy SitumbekoNo ratings yet
- 5-Pelvic Imflamatory DiseasesDocument10 pages5-Pelvic Imflamatory DiseasesTouseeq ManzoorNo ratings yet
- Ureaplasma Infection, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandUreaplasma Infection, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- VaginitisDocument14 pagesVaginitisaisa baladjiNo ratings yet
- Reproductive Tract Infections, Sexual Transmitted Diseases, and HIV in ObstetricDocument58 pagesReproductive Tract Infections, Sexual Transmitted Diseases, and HIV in ObstetricAbdulrahman NajiNo ratings yet
- Sexually Transmitted DiseasesDocument17 pagesSexually Transmitted DiseasesChrystele Ann Ramilo100% (1)
- VaginitisDocument54 pagesVaginitisgloria100% (1)
- Sexually Transmitted Infections GuideDocument89 pagesSexually Transmitted Infections GuidegibreilNo ratings yet
- 54.vaginal DischargeDocument40 pages54.vaginal DischargebenNo ratings yet
- Obstetrics Vaginitis PresentationDocument4 pagesObstetrics Vaginitis PresentationBlue TechNo ratings yet
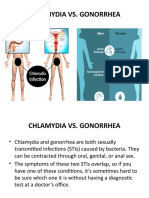
- Chlamydia Vs GonorrhoeaDocument31 pagesChlamydia Vs Gonorrhoeakyro draxNo ratings yet
- WCLfE1j66fYPUTf0149Document165 pagesWCLfE1j66fYPUTf0149ClintonNo ratings yet
- Pelvic Inflammatory DiseaseDocument5 pagesPelvic Inflammatory DiseaseChona JimenezNo ratings yet
- Maternal InfectionsDocument31 pagesMaternal InfectionsJane Ann AlolodNo ratings yet
- Vaginal Discharge Causes and ManagementDocument5 pagesVaginal Discharge Causes and ManagementHassan Abdullah AL-balushiNo ratings yet
- A Simple Guide to Sexually Transmitted DiseasesFrom EverandA Simple Guide to Sexually Transmitted DiseasesRating: 5 out of 5 stars5/5 (9)
- PathophysiologyDocument5 pagesPathophysiologyJessyl GirayNo ratings yet
- PRESENTATION ON STI'sDocument52 pagesPRESENTATION ON STI'sEBENEZER OPPONGNo ratings yet
- Pelvic Inflammatory Disease GuideDocument5 pagesPelvic Inflammatory Disease GuideRahma Rafina100% (2)
- Management of Persistent Vaginitis .99281 PDFDocument12 pagesManagement of Persistent Vaginitis .99281 PDFWinna Eka PNo ratings yet
- Sexually Transmitted Infections-5Document5 pagesSexually Transmitted Infections-5diko_nalNo ratings yet
- STD Family Medicine-WPS OfficeDocument25 pagesSTD Family Medicine-WPS OfficeJs JsNo ratings yet
- Anti-Yeast Diet: A Beginner's 2-Week Step-by-Step for Women, with Curated Recipes and a Sample Meal PlanFrom EverandAnti-Yeast Diet: A Beginner's 2-Week Step-by-Step for Women, with Curated Recipes and a Sample Meal PlanNo ratings yet
- Anti-Yeast Diet for Women: A Beginner's 2-Week Step-by-Step for Women, with Curated Recipes and a Sample Meal PlanFrom EverandAnti-Yeast Diet for Women: A Beginner's 2-Week Step-by-Step for Women, with Curated Recipes and a Sample Meal PlanNo ratings yet
- Pelvic Inflammatory Disease - EditedDocument7 pagesPelvic Inflammatory Disease - EditedDanNo ratings yet
- The Complications of Unprotected SexDocument33 pagesThe Complications of Unprotected Seximi ridleyNo ratings yet
- Vaginitis and Vaginal DischargeDocument52 pagesVaginitis and Vaginal Dischargedrdoaabakhet148No ratings yet
- STIs: Facts, Causes and PreventionDocument48 pagesSTIs: Facts, Causes and PreventionJean Gwyneth Gatchalian100% (1)
- Sexually Transmitted Diseases and Methods of ContraceptionDocument62 pagesSexually Transmitted Diseases and Methods of Contraceptionhohmannjasmin65No ratings yet
- Vaginal Discharge Causes and TreatmentsDocument14 pagesVaginal Discharge Causes and TreatmentsMsharaniaNo ratings yet
- Sexually Transmitted Infections and PregnancyDocument19 pagesSexually Transmitted Infections and PregnancyBeyins TiuNo ratings yet
- n368 Gyn Presentation - StisDocument37 pagesn368 Gyn Presentation - Stisapi-508266867No ratings yet
- Sexually Transmitted Infections (STIs)Document11 pagesSexually Transmitted Infections (STIs)Ester PeregrinaNo ratings yet
- Bacteسيبليسليسl genital tract infectionsDocument60 pagesBacteسيبليسليسl genital tract infectionsDr.Issam JumaaNo ratings yet
- 3 Percent: Ivy Marie R. Maratas BSED Mathematics 1-2 Understanding The Self (GE 1)Document8 pages3 Percent: Ivy Marie R. Maratas BSED Mathematics 1-2 Understanding The Self (GE 1)Ivy Marie MaratasNo ratings yet
- Vulvovaginal InfectionDocument37 pagesVulvovaginal Infectionmadmax500No ratings yet
- Vaginitis BartolinitisDocument28 pagesVaginitis Bartolinitisfani kurniaNo ratings yet
- Jurnal VaginitisDocument8 pagesJurnal VaginitisKariina Indah PrayogiNo ratings yet
- B04801007013 PDFDocument7 pagesB04801007013 PDFrismahNo ratings yet
- B04801007013 PDFDocument7 pagesB04801007013 PDFrismahNo ratings yet
- B04801007013 PDFDocument7 pagesB04801007013 PDFrismahNo ratings yet
- Reproductive Tract InformationDocument14 pagesReproductive Tract InformationGonçalo BaptistaNo ratings yet
- Sindrome Duh Genital Non GODocument15 pagesSindrome Duh Genital Non GOIntan PermataNo ratings yet
- Gonorrhea: SymptomsDocument9 pagesGonorrhea: Symptomspragna novaNo ratings yet
- Infeksi Genitalia Interna & ExternaDocument63 pagesInfeksi Genitalia Interna & ExternaPoetri IermayaniNo ratings yet
- Urethritis in FemaleDocument7 pagesUrethritis in FemaleRika SuryanaNo ratings yet
- Synonyms Causative Agents Incubatiob Period Mode of Transmission Signs and Symptoms Period of Communicability Diagnostic Test Medical Management Nursing Management ComplicationsDocument13 pagesSynonyms Causative Agents Incubatiob Period Mode of Transmission Signs and Symptoms Period of Communicability Diagnostic Test Medical Management Nursing Management ComplicationsYnah DominiqueNo ratings yet
- Pathogenesis, diagnosis and treatment of vaginitis and cervicitisDocument7 pagesPathogenesis, diagnosis and treatment of vaginitis and cervicitisNisaNo ratings yet
- STDs Report Provides Insight on Chlamydia, Gonorrhea, SyphilisDocument76 pagesSTDs Report Provides Insight on Chlamydia, Gonorrhea, Syphilissomaya abdulhakimNo ratings yet
- Managing PID in Primary CareDocument2 pagesManaging PID in Primary CareManjuNo ratings yet
- GYN 讀書報告Document67 pagesGYN 讀書報告Chia-Yuan ChenNo ratings yet
- Pelvic Inflammatory Disease (Pid)Document42 pagesPelvic Inflammatory Disease (Pid)Aruna PoovalingamNo ratings yet
- (Sexually Transmitted Infections) : By. Mrs. MurtiningsihDocument21 pages(Sexually Transmitted Infections) : By. Mrs. MurtiningsihraiNo ratings yet
- 1 Summarization-Updated (AutoRecovered)Document6 pages1 Summarization-Updated (AutoRecovered)Joan SevillaNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFNur intan cahyaniNo ratings yet
- Sexually Transmitted InfectionsDocument48 pagesSexually Transmitted InfectionsYsabella LlanetaNo ratings yet
- Garlic KhasiatDocument32 pagesGarlic KhasiatRinawati BarusNo ratings yet
- Pros Tho Don Tic Considerations in Diabetes MellitusDocument16 pagesPros Tho Don Tic Considerations in Diabetes MellitusDrPrachi AgrawalNo ratings yet
- Home Remedies For Yeast InfectionDocument9 pagesHome Remedies For Yeast InfectionNiharika DasNo ratings yet
- White Tongue Causes & 10 Natural Treatments For White Tongue - Dr. AxeDocument10 pagesWhite Tongue Causes & 10 Natural Treatments For White Tongue - Dr. AxeRaghuNo ratings yet
- Ob Gyne NotesDocument9 pagesOb Gyne NotesPaul Anthony Lorica100% (1)
- Common Skin Diseases in Africa: An Illustrated GuideDocument85 pagesCommon Skin Diseases in Africa: An Illustrated GuideJohn EnioladeNo ratings yet
- Beximko Annual Report 2013Document97 pagesBeximko Annual Report 2013বিধান রয়No ratings yet
- Rag Mycology Learning ObjectivesDocument5 pagesRag Mycology Learning ObjectivesMaster MastrikerNo ratings yet
- Lesson 1 MycologyDocument12 pagesLesson 1 MycologyMUNDER OMAIRA NASRA D.No ratings yet
- Causative Agent CandidiasisDocument2 pagesCausative Agent CandidiasisDiamante MhayaleneNo ratings yet
- Pediatric Pulmonology Specialty Review and Self-Assessment 4e 40 Sep 1 2015 41 40 B014SEGC0K 41 40 StatPearls Publishing LLC 41Document1,359 pagesPediatric Pulmonology Specialty Review and Self-Assessment 4e 40 Sep 1 2015 41 40 B014SEGC0K 41 40 StatPearls Publishing LLC 41Anas Sheikh ibrahimNo ratings yet
- Epidemiology and Etiology of Denture Stomatitis: KeywordsDocument10 pagesEpidemiology and Etiology of Denture Stomatitis: Keywordsluthfia choirunnisaNo ratings yet
- DeuteromycotaDocument10 pagesDeuteromycotaReeza MegavitryNo ratings yet
- Wild Oregano BrochureDocument2 pagesWild Oregano Brochurerosnie22No ratings yet
- Factors Associated with Invasive Fungal Infections in Multiple Myeloma PatientsDocument4 pagesFactors Associated with Invasive Fungal Infections in Multiple Myeloma PatientsMario ChristopherNo ratings yet
- Vomiting BirdsDocument2 pagesVomiting BirdsJumbosizeNo ratings yet
- Ijcdc: Comparative Efficacy of Tea Tree Oil Nanoemulgel and Tea Tree Oil Gel Against Candida AlbicansDocument6 pagesIjcdc: Comparative Efficacy of Tea Tree Oil Nanoemulgel and Tea Tree Oil Gel Against Candida Albicansal rzNo ratings yet
- Materia Medica Sanum PDFDocument354 pagesMateria Medica Sanum PDFPaulo de OliveiraNo ratings yet
- DERMATOLOGY - Cuteneous Candidiasis, PityrosporumDocument4 pagesDERMATOLOGY - Cuteneous Candidiasis, PityrosporumIsabel CastilloNo ratings yet
- Homeopatie EchinaceeaDocument16 pagesHomeopatie EchinaceeaelenasiraduNo ratings yet
- Metronidazole AFTinfDocument8 pagesMetronidazole AFTinfSmartishag BediakoNo ratings yet
- Oral Medicine MCQs CollectionDocument47 pagesOral Medicine MCQs CollectionBharti KahiNo ratings yet
- Systemic Fungal Infections GuideDocument107 pagesSystemic Fungal Infections GuidePrincewill SeiyefaNo ratings yet
- BodyEcology Cookbook GutSmartDocument192 pagesBodyEcology Cookbook GutSmartsarah100% (2)
- Fungal Infection PicturesDocument26 pagesFungal Infection PicturesAshty RzgarNo ratings yet
- Medicine Chart For ChickensDocument35 pagesMedicine Chart For ChickensJuan Escobar Juncal50% (2)
- Monazol, Ovule Spc-EngDocument6 pagesMonazol, Ovule Spc-EngAhmad Muhammad EmamNo ratings yet
- Causes, Symptoms and Treatments of VaginitisDocument16 pagesCauses, Symptoms and Treatments of VaginitisMae Christelle Hamoy100% (2)
- PCOS HealingDocument36 pagesPCOS HealingKheyrne Danu100% (1)
- Drug Classification - 001Document22 pagesDrug Classification - 001Marigold CortezNo ratings yet