You might also like
- IJRPBSDocument8 pagesIJRPBSrakesh2284No ratings yet
- Reserch Paper - ModifiedDocument16 pagesReserch Paper - ModifiedSushilkumar ShindeNo ratings yet
- Journal of Chemical and Pharmaceutical Research, 2013, 5 (5) :1-11Document11 pagesJournal of Chemical and Pharmaceutical Research, 2013, 5 (5) :1-11NurulnameiiNo ratings yet
- RP-HPLC Method Development and Validation For The Estimation of Diclofenac Sodium, Tramadol Hydrochloride and Chlorzoxazone From Their Combined Tablet Dosage FormDocument6 pagesRP-HPLC Method Development and Validation For The Estimation of Diclofenac Sodium, Tramadol Hydrochloride and Chlorzoxazone From Their Combined Tablet Dosage FormPinak PatelNo ratings yet
- Simultaneous Estimation of Ibuprofen and Famotidine in Pure and Combination Dosage Form by RP-HPLCDocument5 pagesSimultaneous Estimation of Ibuprofen and Famotidine in Pure and Combination Dosage Form by RP-HPLCrajj_2323No ratings yet
- Stability Indicating RP-LC Assay Method For Carisoprodol: Original ArticleDocument7 pagesStability Indicating RP-LC Assay Method For Carisoprodol: Original ArticleNguyen binhNo ratings yet
- Development and Validation of Reversed-Phase HPLC Method For Simultaneous Estimation of Rosuvastatin and Fenofibrate in Tablet Dosage FormDocument6 pagesDevelopment and Validation of Reversed-Phase HPLC Method For Simultaneous Estimation of Rosuvastatin and Fenofibrate in Tablet Dosage FormshraddhaJPNo ratings yet
- Redox Reaction Based Spectrophotometric Assay of Some Drugs in PharmaceuticalsDocument6 pagesRedox Reaction Based Spectrophotometric Assay of Some Drugs in PharmaceuticalsseanNo ratings yet
- PoloDocument3 pagesPoloRaja AbhilashNo ratings yet
- Jurnal InternasionalDocument12 pagesJurnal InternasionalIsra Tri HardiantiNo ratings yet
- Method Development and Validation of RP-HPLCDocument8 pagesMethod Development and Validation of RP-HPLCManuel PardiñaNo ratings yet
- Method validation for simultaneous estimation of Ofloxacin and Ornidazole by RP-HPLCDocument7 pagesMethod validation for simultaneous estimation of Ofloxacin and Ornidazole by RP-HPLCHugo Snchez muñozNo ratings yet
- 1 Reverse HPLC Method BudesonideDocument11 pages1 Reverse HPLC Method Budesonidenonick18No ratings yet
- 20211226124933a5 64 JCM 2108 2174Document11 pages20211226124933a5 64 JCM 2108 2174Venkat PalaganiNo ratings yet
- OutDocument11 pagesOutAngel EivinoNo ratings yet
- Research Article: Received: 23 July 2016, Revised and Accepted: 30 September 2016Document7 pagesResearch Article: Received: 23 July 2016, Revised and Accepted: 30 September 2016AndreyNo ratings yet
- Jurnal Ambroxol 1Document19 pagesJurnal Ambroxol 1Claudia AngelinaNo ratings yet
- Analytical Method Development and Validation of Teneligliptin by Using RP HPLC With ICH GuidelinesDocument5 pagesAnalytical Method Development and Validation of Teneligliptin by Using RP HPLC With ICH GuidelinesEditor IJTSRDNo ratings yet
- Research Journal of Pharmaceutical, Biological and Chemical SciencesDocument11 pagesResearch Journal of Pharmaceutical, Biological and Chemical Sciencesyuna yulianaNo ratings yet
- Validated UV method for Amlodipine, Valsartan and HydrochlorothiazideDocument5 pagesValidated UV method for Amlodipine, Valsartan and Hydrochlorothiazideabdelaziz_ismail685662No ratings yet
- Research PratikshaDocument8 pagesResearch PratikshaNutan Desai RaoNo ratings yet
- Fluorescence PaperDocument15 pagesFluorescence Papernisar khanNo ratings yet
- A Validated RP-HPLC Method For The Determination of Bendamustine Hydrochloride in Tablet Dosage Form Using Gemcitabine Hydrochloride As Internal StandardDocument8 pagesA Validated RP-HPLC Method For The Determination of Bendamustine Hydrochloride in Tablet Dosage Form Using Gemcitabine Hydrochloride As Internal StandardHeidi HughesNo ratings yet
- Bisoprolol StabilityDocument7 pagesBisoprolol StabilityAlinaDianaNo ratings yet
- Nimesulid Spectrofotometric1Document8 pagesNimesulid Spectrofotometric1danielafarmacie_1617No ratings yet
- AttachmentDocument7 pagesAttachmentAsihPuspitaPutriNo ratings yet
- SIMULTANEOUS DETERMINATION OF CETIRIZINE AND AMBROXOLDocument11 pagesSIMULTANEOUS DETERMINATION OF CETIRIZINE AND AMBROXOLNafaqohSalmaRahmawatiNo ratings yet
- STABILITY INDICATING ASSAY METHOD DEVELOPMENT AND VALIDATION OF PREGABALIN IN PHARMACEUTICAL DOSAGE FORMS BY RP-HPLC P.Sneha, Prathima SrinivasDocument10 pagesSTABILITY INDICATING ASSAY METHOD DEVELOPMENT AND VALIDATION OF PREGABALIN IN PHARMACEUTICAL DOSAGE FORMS BY RP-HPLC P.Sneha, Prathima SrinivasiajpsNo ratings yet
- A Simple RP-HPLC Method For Simultaneous Analysis of Pseudoephedrine, Bambuterol, Levocetirizine and Montelukast in Pharmaceutical Dosage FormsDocument9 pagesA Simple RP-HPLC Method For Simultaneous Analysis of Pseudoephedrine, Bambuterol, Levocetirizine and Montelukast in Pharmaceutical Dosage FormsijsidonlineinfoNo ratings yet
- UV method for metformin quantification in tabletsDocument4 pagesUV method for metformin quantification in tabletsWilliam SmithNo ratings yet
- 45 Vol. 11 Issue 9 Sep 2020 IJPSR RA 13228Document8 pages45 Vol. 11 Issue 9 Sep 2020 IJPSR RA 13228foaad foaadNo ratings yet
- 3845-Article Text-10897-2-10-20200114Document5 pages3845-Article Text-10897-2-10-20200114nhan phamNo ratings yet
- Development and Validation of A Simple HPLC Method For Simultaneous in Vitro Determination of Amoxicillin and Metronidazole at Single WavelengthDocument5 pagesDevelopment and Validation of A Simple HPLC Method For Simultaneous in Vitro Determination of Amoxicillin and Metronidazole at Single WavelengthAnkit VishnoiNo ratings yet
- Stability-indicating RP-HPLC method for racecadotril quantificationDocument8 pagesStability-indicating RP-HPLC method for racecadotril quantificationAnjay MalikNo ratings yet
- Stability Indicating RP-HPLC Method For Simultaneous Determination of Glecaprevir and Pibrentasvir in Bulk and Pharmaceutical Dosage FormDocument9 pagesStability Indicating RP-HPLC Method For Simultaneous Determination of Glecaprevir and Pibrentasvir in Bulk and Pharmaceutical Dosage FormsadafNo ratings yet
- AbstractDocument11 pagesAbstractEllie satrianiNo ratings yet
- RP-HPLC Method Development and Validation of Rimonabant Hydrochloride in Bulk and Pharmaceutical Dosage FormsDocument7 pagesRP-HPLC Method Development and Validation of Rimonabant Hydrochloride in Bulk and Pharmaceutical Dosage FormsprkrguhsfbNo ratings yet
- ChlordiazepoxideHydrochlorideClidiniumBromide and PantprazoleDocument6 pagesChlordiazepoxideHydrochlorideClidiniumBromide and Pantprazoleiabureid7460No ratings yet
- Stability Indicating RP-HPLC Method for Drug EstimationDocument15 pagesStability Indicating RP-HPLC Method for Drug EstimationAfonso RobertoNo ratings yet
- A HPLC Method For The Determination of Bisoprolol in Tablets and Its Application To A Bioequivalence StudyDocument5 pagesA HPLC Method For The Determination of Bisoprolol in Tablets and Its Application To A Bioequivalence StudyAlinaDianaNo ratings yet
- RP-HPLC and UV methods for analysis of fluconazole in pharmaceutical solid dosage formsDocument6 pagesRP-HPLC and UV methods for analysis of fluconazole in pharmaceutical solid dosage formsJuan PerezNo ratings yet
- Development and Validation of An RP-HPLC Method For Simultaneous Estimation of Amlodipine Besylate and Indapamide in Bulk and Tablet Dosage FormDocument10 pagesDevelopment and Validation of An RP-HPLC Method For Simultaneous Estimation of Amlodipine Besylate and Indapamide in Bulk and Tablet Dosage FormBaru Chandrasekhar RaoNo ratings yet
- Assay of Atenolol Using Bromate-Bromide and Methyl OrangeDocument11 pagesAssay of Atenolol Using Bromate-Bromide and Methyl Orangeحمزة الفنينيNo ratings yet
- Degradation PramipexoleDocument9 pagesDegradation Pramipexoleclaudiamaniac7No ratings yet
- Validated HPLC Method for Empagliflozin ImpuritiesDocument13 pagesValidated HPLC Method for Empagliflozin Impuritiesmanoj bhattaraiNo ratings yet
- Estabilidad de La IndometacinaDocument7 pagesEstabilidad de La IndometacinaJosé RojasNo ratings yet
- Simultaneous HCTZ + Amlodipine + Losartan HPLC PDFDocument6 pagesSimultaneous HCTZ + Amlodipine + Losartan HPLC PDFNájla KassabNo ratings yet
- Stability Indicating RP-HPLC Method For Simultaneous Determination of Perindopril and Indapamide in Pharmaceutical Dosage FormDocument9 pagesStability Indicating RP-HPLC Method For Simultaneous Determination of Perindopril and Indapamide in Pharmaceutical Dosage FormBoovizhikannan ThangabalanNo ratings yet
- Fast LIBS Analysis of Anti-Diabetic TabletsDocument8 pagesFast LIBS Analysis of Anti-Diabetic Tabletsrayo_mishugalde505No ratings yet
- Research Paper WJPPS - 1Document10 pagesResearch Paper WJPPS - 1Farahat AliNo ratings yet
- LC-MS Method for Quantifying Diabetes DrugDocument13 pagesLC-MS Method for Quantifying Diabetes DrugManishaNo ratings yet
- A Validated RP-HPLC Method For The Determination of Celecoxib in Bulk and Pharmaceutical Dosage FormDocument5 pagesA Validated RP-HPLC Method For The Determination of Celecoxib in Bulk and Pharmaceutical Dosage FormOskar LazaroNo ratings yet
- Development and Validation of RP-HPLC Method For Quantitative Estimation of Indapamide in Bulk and Pharmaceutical Dosage FormsDocument6 pagesDevelopment and Validation of RP-HPLC Method For Quantitative Estimation of Indapamide in Bulk and Pharmaceutical Dosage FormsAlexandru GondorNo ratings yet
- D Jothiewari Et. Al.. (UV)Document5 pagesD Jothiewari Et. Al.. (UV)EVELYN SOLANHS ACERO RODRIGUEZNo ratings yet
- Development and Validation of A Dried Blood Spot LC-MS/MS Assay To Quantify Furosemide in Human Whole Blood: An Approach To Improve The Design of PK Studies in Pediatric Population.Document7 pagesDevelopment and Validation of A Dried Blood Spot LC-MS/MS Assay To Quantify Furosemide in Human Whole Blood: An Approach To Improve The Design of PK Studies in Pediatric Population.IOSRjournalNo ratings yet
- HPLC Method Development and Validation of Combined Dosage Form of Atenolol and Indapamide in TabletsDocument22 pagesHPLC Method Development and Validation of Combined Dosage Form of Atenolol and Indapamide in TabletsRam VijayNo ratings yet
- New RP-HPLC Method For The Determination of Olmesartan Medoxomil in Tablet Dosage FormDocument7 pagesNew RP-HPLC Method For The Determination of Olmesartan Medoxomil in Tablet Dosage FormsanjeevbhatNo ratings yet
- Dissolution Test For Glibenclamide TabletsDocument4 pagesDissolution Test For Glibenclamide TabletsYuda Anzas MaraNo ratings yet
- Practical Handbook of Pharmaceutical Chemistry for M.PharmFrom EverandPractical Handbook of Pharmaceutical Chemistry for M.PharmNo ratings yet
- 2016 Article 59Document9 pages2016 Article 59AlinaDianaNo ratings yet
- LC-MS 1Document7 pagesLC-MS 1AlinaDianaNo ratings yet
- (PDF) Phyto-Functionalized Silver Nanoparticles Derived From Conifer Bark Extracts and Evaluation of Their Antimicrobial and Cytogenotoxic EffectsDocument16 pages(PDF) Phyto-Functionalized Silver Nanoparticles Derived From Conifer Bark Extracts and Evaluation of Their Antimicrobial and Cytogenotoxic EffectsAlinaDianaNo ratings yet
- TramadolDocument8 pagesTramadolAlinaDianaNo ratings yet
- Design, Synthesis, in Silico and in Vitro StudiesDocument32 pagesDesign, Synthesis, in Silico and in Vitro StudiesAlinaDianaNo ratings yet
- Development and Validation of A Method For Quantitative Determination of Amiodarone Hydrochloride in Blood Serum by HPLC-MS-MDocument6 pagesDevelopment and Validation of A Method For Quantitative Determination of Amiodarone Hydrochloride in Blood Serum by HPLC-MS-MAlinaDianaNo ratings yet
- Gaz CromatografiaDocument1 pageGaz CromatografiaAlinaDianaNo ratings yet
- LC-MS 4Document12 pagesLC-MS 4AlinaDianaNo ratings yet
- Noi Derivati de Indometacin Donori de NoDocument21 pagesNoi Derivati de Indometacin Donori de NoEliNo ratings yet
- AlprazolamDocument6 pagesAlprazolamAlinaDianaNo ratings yet
- Determination of Enalapril Maleate From Tablets Using A New HPLC MethodDocument6 pagesDetermination of Enalapril Maleate From Tablets Using A New HPLC MethodAlinaDianaNo ratings yet
- Codul Divin Al VietiiDocument94 pagesCodul Divin Al VietiiAlinaDianaNo ratings yet
- A New High Performance Liquid Chromatographic Analysis Method For CiprofloxacinDocument4 pagesA New High Performance Liquid Chromatographic Analysis Method For CiprofloxacinAlinaDianaNo ratings yet
- Complex Combination of U (VI) With SchiffDocument5 pagesComplex Combination of U (VI) With SchiffAlinaDianaNo ratings yet
- 2018 Congres BucurestiDocument2 pages2018 Congres BucurestiAlinaDianaNo ratings yet
- A New Spectrophotometric Method For The Assay of Lisinopril PDFDocument6 pagesA New Spectrophotometric Method For The Assay of Lisinopril PDFAlinaDianaNo ratings yet
- Design and Study of Electrochemical Sensors Based On Polymer PDFDocument5 pagesDesign and Study of Electrochemical Sensors Based On Polymer PDFAlinaDianaNo ratings yet
- A New Spectrometric Method For Quantitative Determination Through Molecular Absorption of LisinoprilDocument4 pagesA New Spectrometric Method For Quantitative Determination Through Molecular Absorption of LisinoprilAlinaDianaNo ratings yet
- Bibire CiprofloxacinDocument19 pagesBibire CiprofloxacinAlinaDianaNo ratings yet
- CIOCOLATA - ALIMENT. DELICIU SAU DROG2018 Ist Farm Extenso GTDocument6 pagesCIOCOLATA - ALIMENT. DELICIU SAU DROG2018 Ist Farm Extenso GTAlinaDianaNo ratings yet
- A New Method For The Assay of Bisoprolol Using Bromocresol GreenDocument5 pagesA New Method For The Assay of Bisoprolol Using Bromocresol GreenAlinaDianaNo ratings yet
- A HPLC Method For The Determination of Bisoprolol in Tablets and Its Application To A Bioequivalence StudyDocument5 pagesA HPLC Method For The Determination of Bisoprolol in Tablets and Its Application To A Bioequivalence StudyAlinaDianaNo ratings yet
- A New Spectrometric Method For Quantitative Determination Through Molecular Absorption of LisinoprilDocument4 pagesA New Spectrometric Method For Quantitative Determination Through Molecular Absorption of LisinoprilAlinaDianaNo ratings yet
- Antiinflammatory Activity of An N, N'-DisalicylidenemethylendiamineDocument4 pagesAntiinflammatory Activity of An N, N'-DisalicylidenemethylendiamineAlinaDianaNo ratings yet
- Complex Combination of U (VI) With SchiffDocument5 pagesComplex Combination of U (VI) With SchiffAlinaDianaNo ratings yet
- Design and Study of Electrochemical Sensors Based On Polymer PDFDocument5 pagesDesign and Study of Electrochemical Sensors Based On Polymer PDFAlinaDianaNo ratings yet
- Antiinflammatory Activity of An N, N'-DisalicylidenemethylendiamineDocument4 pagesAntiinflammatory Activity of An N, N'-DisalicylidenemethylendiamineAlinaDianaNo ratings yet
- A New Spectrophotometric Method For The Assay of Lisinopril PDFDocument6 pagesA New Spectrophotometric Method For The Assay of Lisinopril PDFAlinaDianaNo ratings yet
- A New High Performance Liquid Chromatographic Analysis Method For CiprofloxacinDocument4 pagesA New High Performance Liquid Chromatographic Analysis Method For CiprofloxacinAlinaDianaNo ratings yet
- A New and Sensitive Method For The Clopidogrel PDFDocument4 pagesA New and Sensitive Method For The Clopidogrel PDFAlinaDianaNo ratings yet
- Trays of Columns PDFDocument16 pagesTrays of Columns PDFamirejazminhassNo ratings yet
- ISO - 15926 14 - 2020 09 READI DeliverableDocument123 pagesISO - 15926 14 - 2020 09 READI DeliverablePower StarNo ratings yet
- Permutations and Combinations Quiz AnswersDocument15 pagesPermutations and Combinations Quiz AnswerslenerNo ratings yet
- Detailed Lesson Plan in Mathematics Grade 7 (Addition of Fractions) I. ObjectivesDocument4 pagesDetailed Lesson Plan in Mathematics Grade 7 (Addition of Fractions) I. ObjectivesRosalina Malig100% (2)
- 5964 4peDocument4 pages5964 4peTERASAT SA100% (1)
- Ranorex TutorialDocument436 pagesRanorex Tutorialpetertzen50% (4)
- 1430 - Golden Altos Nepp 2017 JuneDocument19 pages1430 - Golden Altos Nepp 2017 JuneAylia RizviNo ratings yet
- iCR 3600 Flat Gear and Motor Replacement: WarningDocument13 pagesiCR 3600 Flat Gear and Motor Replacement: WarningEliana Caceres TorricoNo ratings yet
- SynthesisDocument10 pagesSynthesisgudala praveenNo ratings yet
- Manual de Reloj Casio 5183Document1 pageManual de Reloj Casio 5183Miguel Saenz EgúsquizaNo ratings yet
- TestDocument3 pagesTestChristian BernarteNo ratings yet
- Maxwell Equations Rewritten in Differential Forms and Clifford AlgebraDocument8 pagesMaxwell Equations Rewritten in Differential Forms and Clifford AlgebraJames ChapelNo ratings yet
- Es Unit 2 MCQDocument7 pagesEs Unit 2 MCQPradnya NavaleNo ratings yet
- Apache Storm Tutorial PointDocument20 pagesApache Storm Tutorial PointashokmvanjareNo ratings yet
- Framework of The Gorongosaecosystem: K. L. Ti N LeyDocument19 pagesFramework of The Gorongosaecosystem: K. L. Ti N LeyubiNo ratings yet
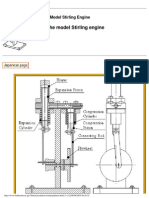
- Plans of The Model Stirling EngineDocument58 pagesPlans of The Model Stirling EngineSemir Muratović100% (3)
- 7 - G10-G20 Series EPSON RobotsDocument11 pages7 - G10-G20 Series EPSON RobotsTaufiq SuyadhiNo ratings yet
- Getting Started With APIs From RPGDocument21 pagesGetting Started With APIs From RPGabercrombieandeNo ratings yet
- ACUDYNE™ LT-120 Hair Fixative Polymer: Maximum Hold With Stiff Feel and Excellent Humidity ResistanceDocument15 pagesACUDYNE™ LT-120 Hair Fixative Polymer: Maximum Hold With Stiff Feel and Excellent Humidity ResistanceKeshav GuptaNo ratings yet
- Windows Se7en XP Black Edition 2010Document4 pagesWindows Se7en XP Black Edition 2010grace natalinNo ratings yet
- Ejercicio Cobol 5Document2 pagesEjercicio Cobol 5MUSICA MUSICANo ratings yet
- RedDragon407 User's ManualDocument20 pagesRedDragon407 User's ManualTavish NarukaNo ratings yet
- Boxer-100-AT-Ktec-1998-2000 AR-BAJAJDocument52 pagesBoxer-100-AT-Ktec-1998-2000 AR-BAJAJJuan Manuel Ortega100% (5)
- Marginal Cost1Document7 pagesMarginal Cost1Randy KempNo ratings yet
- SHA-1 Message Digest AlgorithmDocument16 pagesSHA-1 Message Digest AlgorithmShaheer ArshadNo ratings yet
- Medical: Entrance Exams - 2022Document19 pagesMedical: Entrance Exams - 2022JiyaNo ratings yet
- SPP2021 05 0ContentsReportDocument217 pagesSPP2021 05 0ContentsReportAnton KobrinskyNo ratings yet
- 1 - Lab Schedule (Monday)Document4 pages1 - Lab Schedule (Monday)Mesut OzilNo ratings yet
- Proteus XRa S.MDocument711 pagesProteus XRa S.MМиша ЖигалкинNo ratings yet
- Lesson 6 Quadrilaterals and TrianglesDocument97 pagesLesson 6 Quadrilaterals and TrianglesMarvin Yebes Arce100% (1)