You might also like
- Everthing You Need To Know To Start An Auto DealershipFrom EverandEverthing You Need To Know To Start An Auto DealershipRating: 5 out of 5 stars5/5 (1)
- Motor Accident Report FormDocument4 pagesMotor Accident Report FormLidia MagureanuNo ratings yet
- Reliancegeneral - Co.in 1800 3009 4890 3009: Motor Claim FormDocument4 pagesReliancegeneral - Co.in 1800 3009 4890 3009: Motor Claim FormAL SHEIKHNo ratings yet
- Js by Ms PDFDocument202 pagesJs by Ms PDFMultan Singh BhatiNo ratings yet
- Motor Claim FormDocument2 pagesMotor Claim FormMultan Singh BhatiNo ratings yet
- Unregistered Vehicle PermitDocument2 pagesUnregistered Vehicle PermitJack MartinNo ratings yet
- HDFC ERGO General Insurance Company Limited: Motor Insurance Claim FormDocument4 pagesHDFC ERGO General Insurance Company Limited: Motor Insurance Claim FormNìkhíl HonêyNo ratings yet
- United India Motor Commercial Proposal From PDFDocument2 pagesUnited India Motor Commercial Proposal From PDFRajeev SinghNo ratings yet
- Unregistered Vehicle PemitDocument2 pagesUnregistered Vehicle Pemitmiket241No ratings yet
- Vehicle Accident Report: To Be Completed by The State DriverDocument2 pagesVehicle Accident Report: To Be Completed by The State DriverRomilModiNo ratings yet
- Motor - Claim Form PDFDocument2 pagesMotor - Claim Form PDFarvind gaikwadNo ratings yet
- Here Fold Report of Motor Vehicle Accident: Reset/clearDocument2 pagesHere Fold Report of Motor Vehicle Accident: Reset/clearWashington IrvingNo ratings yet
- Vehicle Accident Claim FormDocument4 pagesVehicle Accident Claim FormLucy WhyteNo ratings yet
- Prrivate Car Proposal Form July 2015Document2 pagesPrrivate Car Proposal Form July 2015Md RashidNo ratings yet
- Private Motor Car Insurance FormDocument5 pagesPrivate Motor Car Insurance FormZila ZiellaNo ratings yet
- Windscreen Claim FormDocument1 pageWindscreen Claim FormHihiNo ratings yet
- PR22005 Car Shield - Private Car Package Policy Proposal Form - Set 1Document4 pagesPR22005 Car Shield - Private Car Package Policy Proposal Form - Set 1Rajiv SethNo ratings yet
- Ac Ko Ac Ko Advant Ag e Advant Ag eDocument5 pagesAc Ko Ac Ko Advant Ag e Advant Ag erakehsNo ratings yet
- Delaware - Applicatio For Title mv212 - Application - For - TitleDocument2 pagesDelaware - Applicatio For Title mv212 - Application - For - TitleSupratik MukhotiNo ratings yet
- XTRAPOWER Application FormDocument5 pagesXTRAPOWER Application FormbiswajitNo ratings yet
- Motor Claim FormDocument4 pagesMotor Claim FormYash SharmaNo ratings yet
- Final Motor Insurance Claim Form Two Aug2018 - 0 PDFDocument1 pageFinal Motor Insurance Claim Form Two Aug2018 - 0 PDFShiva SinghNo ratings yet
- Proposal Form - Motor InsuranceDocument15 pagesProposal Form - Motor InsuranceAbhi PratapNo ratings yet
- FUTURE GENERALI Motor-OD Claim FormDocument1 pageFUTURE GENERALI Motor-OD Claim FormSunetra PalNo ratings yet
- Bond Statement Guide & in Lieu of Bond AffidavitDocument2 pagesBond Statement Guide & in Lieu of Bond Affidavitlane.moreau29No ratings yet
- ArizonaDocument2 pagesArizonaJesus SaenzNo ratings yet
- Proposal FormDocument27 pagesProposal FormChaitanya Chaitu CANo ratings yet
- Future Generali Motor-Od Claim FormDocument2 pagesFuture Generali Motor-Od Claim FormSABodyShop NagpurNo ratings yet
- Zurich Private Car Proposal FormDocument7 pagesZurich Private Car Proposal FormMarcelo Underbeat CarvalhoNo ratings yet
- CreditApplication PDFDocument2 pagesCreditApplication PDFSimbarashe MarisaNo ratings yet
- Your Company Name Repair Order / Invoice: Part No. & Description Qty. AmountDocument1 pageYour Company Name Repair Order / Invoice: Part No. & Description Qty. AmountZakaria AlsyaniyNo ratings yet
- MT RR CG PresentationDocument10 pagesMT RR CG PresentationDave KilbrideNo ratings yet
- Garage Repair Order: Qty Part and Description PriceDocument1 pageGarage Repair Order: Qty Part and Description PriceyordanosnNo ratings yet
- Power of Attorney (Natural Person Only)Document4 pagesPower of Attorney (Natural Person Only)jonkipperNo ratings yet
- Fleet ER DiagramDocument1 pageFleet ER DiagramAnonymous R3BQgOwNo ratings yet
- EGTB Vehicle Inspection Form, 0Document1 pageEGTB Vehicle Inspection Form, 0UstazFaizalAriffinOriginalNo ratings yet
- Motor - Accident Report Form - 30062020Document6 pagesMotor - Accident Report Form - 30062020Gabe LamNo ratings yet
- Laptop All Risk - Insurance Claim FormDocument2 pagesLaptop All Risk - Insurance Claim Formjingyi3889No ratings yet
- Motor Trade Road Risks Quote FormDocument5 pagesMotor Trade Road Risks Quote Formiacovbns1No ratings yet
- Auto Claim FormDocument3 pagesAuto Claim FormdawnNo ratings yet
- 220 31295 Period of Insurance 23 Hneh Do3 To 22-AnDocument4 pages220 31295 Period of Insurance 23 Hneh Do3 To 22-AnDeepNo ratings yet
- Department of State Growth: Application For RegistrationDocument1 pageDepartment of State Growth: Application For Registrationdibesh dhakalNo ratings yet
- Delivery Invoice For CarDocument1 pageDelivery Invoice For Carunclerent2023No ratings yet
- Collision Report Form: A: Other Vehicle OwnerDocument1 pageCollision Report Form: A: Other Vehicle OwnerpodaangoNo ratings yet
- Signed ApplicationDocument4 pagesSigned ApplicationDaBaddest ManagementNo ratings yet
- Motor Insurance - Claim Form: Date of Inward Claim NumberDocument2 pagesMotor Insurance - Claim Form: Date of Inward Claim Numberfabcia llcNo ratings yet
- Zurich Cancellation FormDocument1 pageZurich Cancellation FormKaren MooreNo ratings yet
- Statement of ClaimDocument2 pagesStatement of ClaimRN SantiagoNo ratings yet
- Ogb Commercial Vehicle Loan: Application Form For IndividualsDocument4 pagesOgb Commercial Vehicle Loan: Application Form For IndividualsArun kumar GochhayatNo ratings yet
- Security Code / Report Number / Liable PartyDocument2 pagesSecurity Code / Report Number / Liable PartyRashid HusainNo ratings yet
- Request For Chassis FinancingDocument1 pageRequest For Chassis Financingnodam69776No ratings yet
- Consolidated MVARFDocument2 pagesConsolidated MVARFcherylalsimNo ratings yet
- Final Motor Insurance Claim FormDocument1 pageFinal Motor Insurance Claim FormPrateek PatelNo ratings yet
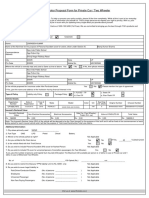
- Motor Proposal Form For Private Car / Two Wheeler: Customer Type: Insured DetailsDocument2 pagesMotor Proposal Form For Private Car / Two Wheeler: Customer Type: Insured DetailsManoj kumar sharmaNo ratings yet
- DMV Form 1799 0805Document2 pagesDMV Form 1799 0805darkhorse35No ratings yet
- MV Tag and or Title Application Form MV1 0Document1 pageMV Tag and or Title Application Form MV1 0Josh SimerNo ratings yet
- 1799 - Vehicle Application (R0118)Document2 pages1799 - Vehicle Application (R0118)sarapreppyhandbookNo ratings yet
- Wrongly Issued PolicyDocument4 pagesWrongly Issued PolicyAfsal JhNo ratings yet
- Etd1848 PDFDocument143 pagesEtd1848 PDFMpho Daniel PuleNo ratings yet
- Eng DFM Marine LeafletDocument1 pageEng DFM Marine LeafletMpho Daniel PuleNo ratings yet
- Grafting Macadamia Trees in Hawai I : Mia Integrifolia) Is One ofDocument6 pagesGrafting Macadamia Trees in Hawai I : Mia Integrifolia) Is One ofMpho Daniel PuleNo ratings yet
- QAS1 TVET - ConsultanciesDocument16 pagesQAS1 TVET - ConsultanciesMpho Daniel PuleNo ratings yet
- Mining Equipment Monitoring & Protection SolutionsDocument12 pagesMining Equipment Monitoring & Protection SolutionsMpho Daniel PuleNo ratings yet
- Eng Mining Presentation v.1.0Document25 pagesEng Mining Presentation v.1.0Mpho Daniel PuleNo ratings yet
- Vehicle Mine StandardDocument4 pagesVehicle Mine StandardMpho Daniel PuleNo ratings yet
- Fleetrun: The Solution For Fleet Maintenance ControlDocument13 pagesFleetrun: The Solution For Fleet Maintenance ControlMpho Daniel PuleNo ratings yet
- Quotation: Pobox808 Gaborone Tel:31932350 F:39332427Document1 pageQuotation: Pobox808 Gaborone Tel:31932350 F:39332427Mpho Daniel PuleNo ratings yet
- Next-Gen Connected Vehicle & Asset Management Technology: 2020 Buyer'S GuideDocument9 pagesNext-Gen Connected Vehicle & Asset Management Technology: 2020 Buyer'S GuideMpho Daniel PuleNo ratings yet
- The Mid Week SUNDocument2 pagesThe Mid Week SUNMpho Daniel PuleNo ratings yet
- Hyundai H 1 BrochureDocument3 pagesHyundai H 1 BrochureMpho Daniel PuleNo ratings yet
- Purchase Orders - B929BFP B581BFRDocument2 pagesPurchase Orders - B929BFP B581BFRMpho Daniel PuleNo ratings yet
- Streets 09-16OCTOBERDocument4 pagesStreets 09-16OCTOBERMpho Daniel PuleNo ratings yet
- Streets 09-16OCTOBERDocument4 pagesStreets 09-16OCTOBERMpho Daniel PuleNo ratings yet
- Minister of Defence, Justice and SecurityDocument10 pagesMinister of Defence, Justice and SecurityMpho Daniel PuleNo ratings yet
- Events 9-16october PDFDocument2 pagesEvents 9-16october PDFMpho Daniel PuleNo ratings yet
- Streets 09-16OCTOBERDocument4 pagesStreets 09-16OCTOBERMpho Daniel PuleNo ratings yet
- View By:: Daily Trip MileageDocument3 pagesView By:: Daily Trip MileageMpho Daniel PuleNo ratings yet
- Speed 09-16OCTOBER PDFDocument2 pagesSpeed 09-16OCTOBER PDFMpho Daniel PuleNo ratings yet
- Speed 09-16OCTOBER PDFDocument2 pagesSpeed 09-16OCTOBER PDFMpho Daniel PuleNo ratings yet
- Speed 09-16OCTOBER PDFDocument2 pagesSpeed 09-16OCTOBER PDFMpho Daniel PuleNo ratings yet
- Events 9-16october PDFDocument2 pagesEvents 9-16october PDFMpho Daniel PuleNo ratings yet
- Events 9-16october PDFDocument2 pagesEvents 9-16october PDFMpho Daniel PuleNo ratings yet
- Quotation: Lease Drive Africa To: QUO001 Botswana RailwaysDocument1 pageQuotation: Lease Drive Africa To: QUO001 Botswana RailwaysMpho Daniel PuleNo ratings yet
- Quotation: Lease Drive Africa To: QUO001 Botswana RailwaysDocument1 pageQuotation: Lease Drive Africa To: QUO001 Botswana RailwaysMpho Daniel PuleNo ratings yet
- Course: We Do One-On-One in Car Training and Not 3, or 2-On-1Document2 pagesCourse: We Do One-On-One in Car Training and Not 3, or 2-On-1Mpho Daniel PuleNo ratings yet
- Tax Invoice: Thank You For Your Business Total 3,910.00Document1 pageTax Invoice: Thank You For Your Business Total 3,910.00Mpho Daniel PuleNo ratings yet
- Quotation: Lease Drive Africa To: QUO001 Botswana RailwaysDocument1 pageQuotation: Lease Drive Africa To: QUO001 Botswana RailwaysMpho Daniel PuleNo ratings yet
- Streets 09-16OCTOBERDocument4 pagesStreets 09-16OCTOBERMpho Daniel PuleNo ratings yet
- Perry I Dr. - Transitions To School PDFDocument301 pagesPerry I Dr. - Transitions To School PDFAdrijana Visnjic JevticNo ratings yet
- Co ownershipQ3ZB2009 PDFDocument4 pagesCo ownershipQ3ZB2009 PDFsting1093No ratings yet
- Chinese Dipping SauceDocument11 pagesChinese Dipping Sauceb.dutta100% (1)
- UML Diagrams Inventory Management SystemDocument10 pagesUML Diagrams Inventory Management SystemSyed Adnan FaroghNo ratings yet
- DowryDocument34 pagesDowryRashid ZubairNo ratings yet
- GRAMMAR POINTS and USEFUL ENGLISHDocument197 pagesGRAMMAR POINTS and USEFUL ENGLISHMiguel Andrés LópezNo ratings yet
- HSM340 Week 4 Homework 1 2 3Document3 pagesHSM340 Week 4 Homework 1 2 3RobynNo ratings yet
- Prodman Part IIDocument14 pagesProdman Part IIVladimir Sabarez LinawanNo ratings yet
- Upstream Pre B1 Unit Test 9Document3 pagesUpstream Pre B1 Unit Test 9Biljana NestorovskaNo ratings yet
- Our Official Guidelines For The Online Quiz Bee Is HereDocument3 pagesOur Official Guidelines For The Online Quiz Bee Is HereAguinaldo Geroy JohnNo ratings yet
- 1 Why The Working Class?: Education For SocialistsDocument32 pages1 Why The Working Class?: Education For SocialistsDrew PoveyNo ratings yet
- Dream Job RequirementsDocument4 pagesDream Job RequirementsOmar AbdulAzizNo ratings yet
- ENTREPRENEURSHIP QuizDocument2 pagesENTREPRENEURSHIP QuizLeona Alicpala100% (2)
- LetterDocument4 pagesLetterapi-247847830No ratings yet
- Service Marketing Notes1 RejinpaulDocument47 pagesService Marketing Notes1 RejinpaulEr. THAMIZHMANI MNo ratings yet
- Lesson 1 Learning History What Is History?Document12 pagesLesson 1 Learning History What Is History?林レッシアNo ratings yet
- G O Ms NoDocument2 pagesG O Ms NoMuralidhar MogalicherlaNo ratings yet
- IELTS Sample Speaking Test 2: Lesson 4Document4 pagesIELTS Sample Speaking Test 2: Lesson 4nọcNo ratings yet
- Reaction PaperDocument3 pagesReaction PaperAnonymous abx5ZiifyNo ratings yet
- CRPC MergedDocument121 pagesCRPC MergedNishal KiniNo ratings yet
- Lease Offer - Flavors - Eggsy PutoDocument7 pagesLease Offer - Flavors - Eggsy PutoThe Seafarer RamNo ratings yet
- Ac3 Permanent File ChecklistDocument4 pagesAc3 Permanent File ChecklistAndrew PanganibanNo ratings yet
- Reviewer For Fundamentals of Accounting and Business ManagementDocument4 pagesReviewer For Fundamentals of Accounting and Business ManagementAngelo PeraltaNo ratings yet
- Summary of Legal Due Diligence Result: Rangkuman Hasil Penelitian HukumDocument2 pagesSummary of Legal Due Diligence Result: Rangkuman Hasil Penelitian HukumErni0684No ratings yet
- Big Data Report 2012Document103 pagesBig Data Report 2012bileshNo ratings yet
- The Dawn of IslamDocument2 pagesThe Dawn of IslamtalhaNo ratings yet
- Family View - Printer Friendly - Ancestry - co.UkPt1Document4 pagesFamily View - Printer Friendly - Ancestry - co.UkPt1faeskeneNo ratings yet
- Jas PDFDocument34 pagesJas PDFJasenriNo ratings yet
- Studying Religion - Russell McCutcheonDocument15 pagesStudying Religion - Russell McCutcheonMuhammad Rizal100% (1)
- OB Escription: Job Title: Delivery DriverDocument2 pagesOB Escription: Job Title: Delivery DriverMarisa Arizky PutriNo ratings yet