You might also like
- Mycology Lab2Document7 pagesMycology Lab2api-3700579100% (1)
- Mycology ReviewDocument9 pagesMycology ReviewChristine NazarenoNo ratings yet
- Laboratory Exercises in Microbiology - Discovering The Unseen WorlDocument208 pagesLaboratory Exercises in Microbiology - Discovering The Unseen WorlJennybabe PartozaNo ratings yet
- Virology: PoisonDocument12 pagesVirology: PoisonArron Piansay Pedrajas100% (2)
- Antibiotic ResistanceDocument32 pagesAntibiotic ResistanceEmine Alaaddinoglu100% (2)
- Practical Manual for Detection of Parasites in Feces, Blood and Urine SamplesFrom EverandPractical Manual for Detection of Parasites in Feces, Blood and Urine SamplesNo ratings yet
- General Mycology 2006-07Document47 pagesGeneral Mycology 2006-07api-3699361100% (5)
- Medical MicrobiologyDocument41 pagesMedical Microbiologyapi-1991639950% (2)
- Microbiology and ParasitologyDocument14 pagesMicrobiology and Parasitologymadam joyNo ratings yet
- Bacteriology Handouts From Sir PalmaresDocument30 pagesBacteriology Handouts From Sir PalmaresTin BabistaNo ratings yet
- Antibiotics & Antibiotic ResistanceDocument53 pagesAntibiotics & Antibiotic ResistanceLeenoos RayapanNo ratings yet
- Microbiology: Higher Secondary-First YearDocument140 pagesMicrobiology: Higher Secondary-First Yearwiranchana-na3014100% (3)
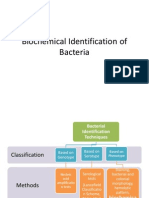
- Biochemical Identification of BacteriaDocument72 pagesBiochemical Identification of BacteriaMaria Jhoyce MagpantayNo ratings yet
- Lecture 11 - Antimicrobial ChemotherapyDocument24 pagesLecture 11 - Antimicrobial Chemotherapyapi-3703352100% (2)
- Medical MicrobiologyDocument63 pagesMedical MicrobiologyDennis Christopher Alfred SajoNo ratings yet
- Microbiology Quiz: Answer All Questions in Two Minutes To Win A Lollypop!Document13 pagesMicrobiology Quiz: Answer All Questions in Two Minutes To Win A Lollypop!SwaraNo ratings yet
- Parasitology Lec ReviewerDocument10 pagesParasitology Lec ReviewerPatricia Ann JoseNo ratings yet
- General Microbiology (Chapter 3)Document18 pagesGeneral Microbiology (Chapter 3)Ashraf OsmanNo ratings yet
- MicrobiologyDocument44 pagesMicrobiologyBonnie Hardy100% (1)
- ANTIMICROBIAL ResistanceDocument4 pagesANTIMICROBIAL ResistancePuspa Das100% (1)
- Lab 01 - Streaking For Isolation and Interpreting Primary Culture ResultsDocument18 pagesLab 01 - Streaking For Isolation and Interpreting Primary Culture ResultsVincent ReyesNo ratings yet
- BacteriologyDocument5 pagesBacteriologyana delos santosNo ratings yet
- Introduction To ParasitologyDocument79 pagesIntroduction To ParasitologyLeeShauran100% (7)
- Microbio Lec 1 - Bacterial Morphology and Ultra StructureDocument8 pagesMicrobio Lec 1 - Bacterial Morphology and Ultra Structureapi-3743217100% (3)
- ParasitologyDocument27 pagesParasitologyDreyden HaloNo ratings yet
- Introduction To MycologyDocument26 pagesIntroduction To MycologyOsannah Irish InsongNo ratings yet
- BacteriologyDocument11 pagesBacteriologyCarmelle Zia Reyes100% (1)
- Medical MicrobiologyDocument82 pagesMedical MicrobiologyAdithya100% (2)
- MycologyDocument26 pagesMycologySkandi43No ratings yet
- Histology Laboratory Manual: Olgga A. Hara MSDocument77 pagesHistology Laboratory Manual: Olgga A. Hara MSMark LopezNo ratings yet
- Anaerobic Bacteria: Dept. of Microbiology Medical Faculty, Padjadjaran UniversityDocument52 pagesAnaerobic Bacteria: Dept. of Microbiology Medical Faculty, Padjadjaran UniversitySabrina Indri WardaniNo ratings yet
- Introduction To MicrobiologyDocument4 pagesIntroduction To MicrobiologyCrazybiologist245No ratings yet
- Chpater 1 MicrobiologyDocument7 pagesChpater 1 MicrobiologyRoma Blaise G FloresNo ratings yet
- Medical Microbiology ReviewerDocument3 pagesMedical Microbiology ReviewerJoan BularioNo ratings yet
- Mycology NotesDocument106 pagesMycology NotesRia Alcantara100% (2)
- A. Staphylococcus Aureus B. Staphylococcus Epidermidis C. Staphylococcus SaprophyticusDocument8 pagesA. Staphylococcus Aureus B. Staphylococcus Epidermidis C. Staphylococcus SaprophyticusRuel MaddawinNo ratings yet
- Man Meets Microbes: An Introduction to Medical MicrobiologyFrom EverandMan Meets Microbes: An Introduction to Medical MicrobiologyNo ratings yet
- BacteriologyDocument75 pagesBacteriologyHoward BarlomentoNo ratings yet
- The Immune SystemDocument15 pagesThe Immune SystemAslak Torgersen100% (1)
- Morphology of Filamentous FungiDocument26 pagesMorphology of Filamentous FungiKathreen Rodriguez DimalibotNo ratings yet
- Microbiology ReviewerDocument8 pagesMicrobiology ReviewerSteph Vee100% (6)
- Microbiology Question PapersDocument100 pagesMicrobiology Question Papersprinceej92% (13)
- MEDICAL MYCOLOGY Dr. Caligagan 2017 HP PDFDocument23 pagesMEDICAL MYCOLOGY Dr. Caligagan 2017 HP PDFROSEMARIE ONGNo ratings yet
- Lecture Notes BacteriologyDocument138 pagesLecture Notes BacteriologyJunalyn Banawe Ocden100% (2)
- Introduction To MicrobiologyDocument27 pagesIntroduction To MicrobiologyNicoel67% (3)
- Importance of MicrobiologyDocument3 pagesImportance of MicrobiologyNathalieCaraca100% (1)
- Tests For Identification of Bacteria ASSDocument4 pagesTests For Identification of Bacteria ASSkrisNo ratings yet
- Mycology Lab1tableDocument6 pagesMycology Lab1tableapi-3700579100% (1)
- Human Parasitology Laboratory (Biol546) : Biology 546 Laboratory Manual - 2012 (.PDF Edition)Document41 pagesHuman Parasitology Laboratory (Biol546) : Biology 546 Laboratory Manual - 2012 (.PDF Edition)Diana ReveloNo ratings yet
- MicrobiologyDocument9 pagesMicrobiologyWenxinn JCFNo ratings yet
- Evaluation Criteria For Family Case StudyDocument2 pagesEvaluation Criteria For Family Case StudySandeep KumarNo ratings yet
- Evaluation Health TalkDocument1 pageEvaluation Health TalkSandeep KumarNo ratings yet
- Presentation IPC-PPE-COVID19-eng PDFDocument42 pagesPresentation IPC-PPE-COVID19-eng PDFYan Gabriel Morais David SilvaNo ratings yet
- Family Health Survey PDFDocument5 pagesFamily Health Survey PDFSandeep KumarNo ratings yet
- Universal Precaution WhoDocument2 pagesUniversal Precaution WhoYayu PujiNo ratings yet
- FAMILY CaseDocument10 pagesFAMILY CaseSandeep KumarNo ratings yet
- CommunicationDocument3 pagesCommunicationSandeep KumarNo ratings yet
- Community Health Nursing FCPDocument4 pagesCommunity Health Nursing FCPSandeep KumarNo ratings yet
- Family FolderDocument5 pagesFamily FolderSandeep Kumar67% (3)
- QuestionDocument16 pagesQuestionSandeep KumarNo ratings yet
- CHN QuestionDocument4 pagesCHN QuestionSandeep KumarNo ratings yet
- Personality 12603021986156 Phpapp02Document28 pagesPersonality 12603021986156 Phpapp02Sandeep KumarNo ratings yet
- Cenetral Pollution Control BoardDocument17 pagesCenetral Pollution Control BoardSandeep KumarNo ratings yet
- Admission of Client To HospitalDocument6 pagesAdmission of Client To HospitalSandeep Kumar100% (1)
- Short Essay On Personality!Document2 pagesShort Essay On Personality!dorathiNo ratings yet
- Committes of Health in IndiaDocument5 pagesCommittes of Health in IndiaRaghavendr Kore100% (1)
- Subject Plan B.SC Nursing 1 Year: MicrobiologyDocument2 pagesSubject Plan B.SC Nursing 1 Year: MicrobiologySandeep KumarNo ratings yet
- EvaluationDocument46 pagesEvaluationSandeep KumarNo ratings yet
- EvaluationDocument46 pagesEvaluationSandeep KumarNo ratings yet
- EpidemiologyDocument1 pageEpidemiologySandeep KumarNo ratings yet
- Role CarrDocument58 pagesRole CarrSandeep KumarNo ratings yet
- Personality Nursing NotesDocument67 pagesPersonality Nursing NotesSandeep KumarNo ratings yet
- Concepts, Determinants and Promotion of HealthDocument30 pagesConcepts, Determinants and Promotion of HealthSandeep KumarNo ratings yet
- 43911Document51 pages43911Ayesha KhalidNo ratings yet
- 9-Reproductive HealthDocument32 pages9-Reproductive HealthLiezel CauilanNo ratings yet
- Assesment of The Reproductive SystemDocument56 pagesAssesment of The Reproductive SystemSandeep KumarNo ratings yet
- NMH Resources CBR Vellore ExperienceDocument15 pagesNMH Resources CBR Vellore ExperienceSandeep KumarNo ratings yet
- 10 09 04 CardiovascularDocument44 pages10 09 04 CardiovascularDesi EryonNo ratings yet
- English 2nd Year NotesDocument18 pagesEnglish 2nd Year NotesMuhammad Irfan Khan100% (4)
- Micro Biology EMDocument320 pagesMicro Biology EMdeliciaammuNo ratings yet
- Biography of Alexander FlemingDocument3 pagesBiography of Alexander FlemingElizabeth Ramos SayritupacNo ratings yet
- (Tailieuvui - Com) 30 de Luyen Thi Vao Lop 10 Mon Tieng AnhDocument162 pages(Tailieuvui - Com) 30 de Luyen Thi Vao Lop 10 Mon Tieng AnhMan NguyenNo ratings yet
- Azim Premji's Speech at IIM AhemdabadDocument3 pagesAzim Premji's Speech at IIM AhemdabadAjayKhandelwalNo ratings yet
- Alexander Fleming BiographyDocument3 pagesAlexander Fleming BiographySocial SinghNo ratings yet
- (AC-S07) Week 07 - Pre-Task - Quiz - Weekly Quiz - INGLES IV (28880) .2Document4 pages(AC-S07) Week 07 - Pre-Task - Quiz - Weekly Quiz - INGLES IV (28880) .2karina salazar huayascachiNo ratings yet
- 2017 Grade 6 Eng Ss His QPDocument9 pages2017 Grade 6 Eng Ss His QPShane KalakgosiNo ratings yet
- READING KEY - Short Answer Questions - Summary - Matching HeadingsDocument10 pagesREADING KEY - Short Answer Questions - Summary - Matching HeadingsMi DoNo ratings yet
- The Story of PenicillimDocument6 pagesThe Story of PenicillimJess Carreño CamargoNo ratings yet
- Rice Genome ProjectDocument20 pagesRice Genome ProjectRanjith MuralidharanNo ratings yet
- Savio Sibi - PharmaChem-1Document11 pagesSavio Sibi - PharmaChem-1Savio SibiNo ratings yet
- 80 de Thi Vao Lop 10 Mon Tieng AnhDocument265 pages80 de Thi Vao Lop 10 Mon Tieng AnhMinh LêNo ratings yet
- English TestsDocument80 pagesEnglish TestsLim BlakeNo ratings yet
- Last Minute Revision English (2023-24)Document189 pagesLast Minute Revision English (2023-24)Prastooti RoyNo ratings yet
- English Test For Wbcs Prelims 2017 Part One: Grammar: WWW - Wbcsmadeeasy.inDocument10 pagesEnglish Test For Wbcs Prelims 2017 Part One: Grammar: WWW - Wbcsmadeeasy.insunny_8206No ratings yet
- Student's WorksheetDocument10 pagesStudent's WorksheetAnh Nguyen DucNo ratings yet
- Summarizing and ParaphrasingDocument12 pagesSummarizing and ParaphrasingNur HafsaNo ratings yet
- Module 1 Introduction To STS Science Technology and SocietypdfDocument14 pagesModule 1 Introduction To STS Science Technology and SocietypdfOwenNo ratings yet
- Inventions of The 20th Century That Changed The WorldDocument3 pagesInventions of The 20th Century That Changed The Worldfoxy LupuNo ratings yet
- Đáp án 30 đề thi THCS lớp 9Document42 pagesĐáp án 30 đề thi THCS lớp 9Chich ChoeNo ratings yet
- CC 202014 20us6r 20ri 20se 20ia1Document8 pagesCC 202014 20us6r 20ri 20se 20ia1api-292667474No ratings yet
- Alexander FlemingDocument10 pagesAlexander FlemingA. DuqueNo ratings yet
- 30 de Luyen Thi Mon Tieng AnhDocument126 pages30 de Luyen Thi Mon Tieng AnhLy UyểnNo ratings yet
- Research Methodology and BiostatisticsDocument163 pagesResearch Methodology and BiostatisticsLourdesNo ratings yet
- PenicillinDocument75 pagesPenicillinJean CabigaoNo ratings yet
- Test Bank For Pharmacy Technician Principles and Practice 3rd Edition HopperDocument24 pagesTest Bank For Pharmacy Technician Principles and Practice 3rd Edition Hopperjenniferhoustonmjcfngpbow100% (42)
- завдання для олімпіади з англійської мови 8-11 класиDocument13 pagesзавдання для олімпіади з англійської мови 8-11 класиOlena KhrapchynskaNo ratings yet
- HPSSB Allied Exam Answer Key Errors 2013 Matter To CMDocument19 pagesHPSSB Allied Exam Answer Key Errors 2013 Matter To CMVIJAY KUMAR HEERNo ratings yet
- The Greatest Invention of All TimeDocument10 pagesThe Greatest Invention of All Timeira boikoNo ratings yet