You might also like
- REPAIR DAN REGENERASI Jaringan LunakDocument48 pagesREPAIR DAN REGENERASI Jaringan LunakCarabelli23 FKG Hang TuahNo ratings yet
- Penyembuhan LukaDocument22 pagesPenyembuhan LukaHaqiqi Amira Syathir100% (1)
- Prinsip Dan Kaidah Perawatan Luka ModernDocument9 pagesPrinsip Dan Kaidah Perawatan Luka ModernIlham HabibNo ratings yet
- PENGOBATAN LUKADocument3 pagesPENGOBATAN LUKALusi RustinaNo ratings yet
- Pemulihan Jaringan - Kelompok 4 - 22A11Document20 pagesPemulihan Jaringan - Kelompok 4 - 22A11Attina Salsa BillaNo ratings yet
- Wound Healing, Skin Graft and Flap WordDocument36 pagesWound Healing, Skin Graft and Flap WordGaluh Ajeng LaraswatiNo ratings yet
- Dasar PenyembuhanDocument4 pagesDasar PenyembuhanAjang TaniarNo ratings yet
- Penyembuhan LukaDocument31 pagesPenyembuhan Lukaulfa dwi intanNo ratings yet
- Penyembuhan LukaDocument4 pagesPenyembuhan LukanadaNo ratings yet
- Proses Penyembuhan LukaDocument9 pagesProses Penyembuhan LukaAndiTiwsNo ratings yet
- Penggunaan Negative Pressure Wound Therapy Pada Luka KronisDocument18 pagesPenggunaan Negative Pressure Wound Therapy Pada Luka KronisArga Putra PradanaNo ratings yet
- WOUND HEALINGDocument14 pagesWOUND HEALINGFebriyanti TkNo ratings yet
- Moist Wound Healing PrintDocument13 pagesMoist Wound Healing PrintLaily AufklarungNo ratings yet
- Penyembuhan Luka Jaringan LunakDocument10 pagesPenyembuhan Luka Jaringan LunakrachmadyNo ratings yet
- Proses Pembentukan Jaringan Granulasi Dalam Penyembuhan LukaDocument12 pagesProses Pembentukan Jaringan Granulasi Dalam Penyembuhan LukaTryani Walnizam100% (1)
- Proses Penyembuhan LukaDocument10 pagesProses Penyembuhan Lukacindy eysiaNo ratings yet
- Proses Penyembuhan LukaDocument6 pagesProses Penyembuhan LukaTri WahayuNo ratings yet
- Proses Penyembuhan LukaDocument9 pagesProses Penyembuhan LukaAmira NaufallNo ratings yet
- Luka Dan Manajemen LukaDocument8 pagesLuka Dan Manajemen LukaLuna Fitria KusumaNo ratings yet
- Penyembuhan Luka Post OperasiDocument15 pagesPenyembuhan Luka Post Operasianggun pratissaNo ratings yet
- Bab IiDocument27 pagesBab IiArfan yutuberNo ratings yet
- 1] Bab 1 Pendahuluan Penyembuhan LukaDocument9 pages1] Bab 1 Pendahuluan Penyembuhan Lukaanisarahma718100% (3)
- Perawatan LukaDocument11 pagesPerawatan LukaayuNo ratings yet
- TP VulnusDocument29 pagesTP VulnusIgaMasPutriNo ratings yet
- Luka Post Op 2021Document46 pagesLuka Post Op 2021cindy claudiaNo ratings yet
- Proses Penyembuhan LukaDocument9 pagesProses Penyembuhan LukaAkbar TaufikNo ratings yet
- Jenis Pilihan Pembalut Luka Terkini 1123Document5 pagesJenis Pilihan Pembalut Luka Terkini 1123FelixLeonardNo ratings yet
- TUGAS KONSEP WOUND Care 11Document4 pagesTUGAS KONSEP WOUND Care 11Rani YunitaNo ratings yet
- Etiologi LukaDocument7 pagesEtiologi LukaHerlina HusenNo ratings yet
- Pemulihan JaringanDocument2 pagesPemulihan Jaringannadiavidira100% (1)
- LP Wound Dehiscence CicilDocument11 pagesLP Wound Dehiscence Ciciljangnoesa100% (2)
- WOUND CARE (1) IyuDocument25 pagesWOUND CARE (1) IyuMaesharah RosyadiNo ratings yet
- Desti Lestari 1a Pato Penyembuhan LukaDocument5 pagesDesti Lestari 1a Pato Penyembuhan Lukadesti lestariNo ratings yet
- Patologi Umum PenyembuhanDocument22 pagesPatologi Umum PenyembuhanAndri SaputraNo ratings yet
- PENYEMBUHAN LUKADocument6 pagesPENYEMBUHAN LUKAWinda AnastesyaNo ratings yet
- Biologi Molekuler Proses Penyembuhan LukaDocument11 pagesBiologi Molekuler Proses Penyembuhan LukaErinne DefrianiNo ratings yet
- Tipe Penyembuhan Luka Dan Mekanisme Penyembuhan LukaDocument4 pagesTipe Penyembuhan Luka Dan Mekanisme Penyembuhan LukaMonica ChristabelNo ratings yet
- Perawatan Luka RiaDocument51 pagesPerawatan Luka RiaDonny SaputraNo ratings yet
- Luka dan PerawatanDocument23 pagesLuka dan PerawatanDien IsnainiNo ratings yet
- Proses Penyembuhan LukaDocument3 pagesProses Penyembuhan Lukabogaga baguguNo ratings yet
- Step Ladder Rekontruksi Dan Wound HealingDocument18 pagesStep Ladder Rekontruksi Dan Wound HealingRizky CaranggonoNo ratings yet
- Repair JaringanDocument2 pagesRepair JaringanAnindya RoshidaNo ratings yet
- Bacaan Rawat LukaDocument7 pagesBacaan Rawat LukaLittle MummutNo ratings yet
- Tugas P. Luka - Anik Ana-WPS Office PDFDocument2 pagesTugas P. Luka - Anik Ana-WPS Office PDFAnikAnafilahNo ratings yet
- Cara Melakukan Perawatan LukaDocument18 pagesCara Melakukan Perawatan LukaseptyNo ratings yet
- Laporan Kasus VulnusDocument14 pagesLaporan Kasus VulnusRimasari Istiqomah Polhaupessy100% (2)
- Perawatan Luka AnakDocument6 pagesPerawatan Luka AnakPutu RereNo ratings yet
- Laporan Tugas Enterpreneur Rawat Luka - Anik BudiartiDocument17 pagesLaporan Tugas Enterpreneur Rawat Luka - Anik BudiartiZogie Ari EffendiNo ratings yet
- HEALINGDocument48 pagesHEALINGIrfan Darul MuttaqinNo ratings yet
- Perawatan LukaDocument24 pagesPerawatan LukamufiaNo ratings yet
- Wound HealingDocument28 pagesWound HealingMaheer JoefrieNo ratings yet
- Proses Penyembuhan LukaDocument7 pagesProses Penyembuhan LukaIpul Bebek Adus KaliNo ratings yet
- Laporan BBDM SKENARIO 1Document4 pagesLaporan BBDM SKENARIO 1Nida CikaNo ratings yet
- Penatalaksanaan Perawatan LukaDocument16 pagesPenatalaksanaan Perawatan LukaAidaFitriaNo ratings yet
- Imunologi Penyembuhan LukaDocument23 pagesImunologi Penyembuhan LukaardirakunNo ratings yet
- Lampiran Pengumuman Cpns 2018 2019Document20 pagesLampiran Pengumuman Cpns 2018 2019Muhammad Purnama AlamNo ratings yet
- Makalah P2M DBDDocument35 pagesMakalah P2M DBDMuziburrahman Irul MbozoNo ratings yet
- Hidup Tanpa Tantangan Tidak Patut Untuk DijalaniDocument3 pagesHidup Tanpa Tantangan Tidak Patut Untuk DijalaniMuziburrahman Irul MbozoNo ratings yet
- Pengorganisasian Dan PenggerakanDocument39 pagesPengorganisasian Dan PenggerakanMuziburrahman Irul MbozoNo ratings yet
- Asuhan Keperawatan CKDDocument39 pagesAsuhan Keperawatan CKDMuziburrahman Irul MbozoNo ratings yet
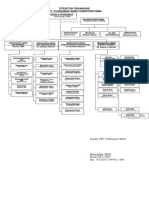
- 2.3.3. EP2 Struktur Organisasi PKM WawoDocument1 page2.3.3. EP2 Struktur Organisasi PKM WawoMuziburrahman Irul MbozoNo ratings yet
- Bab 8-10Document15 pagesBab 8-10Muziburrahman Irul MbozoNo ratings yet
- Pengantar Ilmu Kedokteran TropisDocument4 pagesPengantar Ilmu Kedokteran TropisMuziburrahman Irul MbozoNo ratings yet
- Leaflet SNMPTN 2018Document2 pagesLeaflet SNMPTN 2018agus hariyantoNo ratings yet
- SPSS Transformasi DataDocument12 pagesSPSS Transformasi DataErlangga Jihadul FisabilNo ratings yet
- Organisasi PuskesmasDocument16 pagesOrganisasi PuskesmasMuziburrahman Irul MbozoNo ratings yet
- Kebijakan Akedemik Prodi Ikt 151113 1Document14 pagesKebijakan Akedemik Prodi Ikt 151113 1Muziburrahman Irul MbozoNo ratings yet
- Format Pendaftaran Mawapres 2015Document4 pagesFormat Pendaftaran Mawapres 2015Muziburrahman Irul MbozoNo ratings yet
- Apoptosis Pada Artritis RematoidDocument4 pagesApoptosis Pada Artritis RematoidMuziburrahman Irul MbozoNo ratings yet
- Kedokteran TropisDocument3 pagesKedokteran TropisMuziburrahman Irul MbozoNo ratings yet
- StreptomisinDocument8 pagesStreptomisindanzbroNo ratings yet
- Artritis ReumatoidDocument15 pagesArtritis ReumatoidMuziburrahman Irul MbozoNo ratings yet
- Apoptosis Pada Artritis RematoidDocument4 pagesApoptosis Pada Artritis RematoidMuziburrahman Irul MbozoNo ratings yet
- Tugas Ujian MP Bios Adi WasisDocument14 pagesTugas Ujian MP Bios Adi WasisMuziburrahman Irul MbozoNo ratings yet
- Kewirausahaan dan Pengembangan Profesi HMIDocument1 pageKewirausahaan dan Pengembangan Profesi HMIMuziburrahman Irul MbozoNo ratings yet
- Tugas Ujian MP Bios Adi WasisDocument14 pagesTugas Ujian MP Bios Adi WasisMuziburrahman Irul MbozoNo ratings yet
- Buletin Diare FinalDocument44 pagesBuletin Diare FinalCynthia Dewi Maharani100% (1)
- Analisis Korelasi dan RegresiDocument20 pagesAnalisis Korelasi dan RegresiMuziburrahman Irul MbozoNo ratings yet
- Proposal Terapi Bermain Bona 1Document23 pagesProposal Terapi Bermain Bona 1Muziburrahman irulNo ratings yet
- ANALISIS HUBUNGANDocument15 pagesANALISIS HUBUNGANMuziburrahman Irul MbozoNo ratings yet
- Makalah Regresi Dan Korelasi SederhanaDocument16 pagesMakalah Regresi Dan Korelasi SederhanaKgs Muhammad Reza ArdhiansyahNo ratings yet
- Analisis Korelasi dan RegresiDocument20 pagesAnalisis Korelasi dan RegresiMuziburrahman Irul MbozoNo ratings yet
- Makalah Regresi Dan Korelasi SederhanaDocument16 pagesMakalah Regresi Dan Korelasi SederhanaKgs Muhammad Reza ArdhiansyahNo ratings yet
- Sekolah dan Rekan Sejawat Guru Sebagai Sumber BelajarDocument2 pagesSekolah dan Rekan Sejawat Guru Sebagai Sumber BelajarNoryda Sastriyani100% (2)
- Bab IiiDocument5 pagesBab IiiMuziburrahman Irul MbozoNo ratings yet





















![1] Bab 1 Pendahuluan Penyembuhan Luka](https://imgv2-2-f.scribdassets.com/img/document/263062667/149x198/cfbac270ce/1713188848?v=1)