You might also like
- 2017-2018 Winter Apparel PolicyDocument1 page2017-2018 Winter Apparel PolicyAmyNo ratings yet
- Naa Esa Toolkit 2017Document68 pagesNaa Esa Toolkit 2017AmyNo ratings yet
- Physical Verification Form: Wellness Screen/Annual PhysicalDocument1 pagePhysical Verification Form: Wellness Screen/Annual PhysicalAmyNo ratings yet
- 2017-2018 Winter Apparel PolicyDocument1 page2017-2018 Winter Apparel PolicyAmyNo ratings yet
- October Safety FlyerDocument2 pagesOctober Safety FlyerAmyNo ratings yet
- July Safety NewsletterDocument2 pagesJuly Safety NewsletterAmyNo ratings yet
- Linden Place Grand OpeningDocument2 pagesLinden Place Grand OpeningAmyNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Pharmacy Laws, Medicare, Medicaid and Business Management: Copy Right ProtectedDocument8 pagesPharmacy Laws, Medicare, Medicaid and Business Management: Copy Right Protectedasas100% (1)
- Complete Material SRI 111 CCPDocument51 pagesComplete Material SRI 111 CCPAnimesh Sen50% (2)
- Bloom Insurance Agency 2019 Part C and Part D CMS QuestionsDocument23 pagesBloom Insurance Agency 2019 Part C and Part D CMS QuestionsAmi MoiNo ratings yet
- Boe Agenda 2012 06 05Document532 pagesBoe Agenda 2012 06 05transparentnevadaNo ratings yet
- CMS Financial Report For Fiscal Year 2022Document132 pagesCMS Financial Report For Fiscal Year 2022Russ LatinoNo ratings yet
- The High Cost of Prescriptions - JAMADocument26 pagesThe High Cost of Prescriptions - JAMAamp0201No ratings yet
- Contracted PBM Listing and Contact InformationDocument5 pagesContracted PBM Listing and Contact InformationRao Arslan RajputNo ratings yet
- Sbo - Health Insurance Rates Fy17.18Document1 pageSbo - Health Insurance Rates Fy17.18maria31691No ratings yet
- 1-15 A12060 HMO Manual PDFDocument460 pages1-15 A12060 HMO Manual PDFsyunamiNo ratings yet
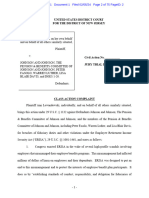
- J&J - Employee Drug Plan SuitDocument74 pagesJ&J - Employee Drug Plan SuitJakob EmersonNo ratings yet
- 2011 CMS Marketing GuidelinesDocument200 pages2011 CMS Marketing Guidelinespoopoodoodoo1No ratings yet
- Healthcare Trends in AmericaDocument101 pagesHealthcare Trends in Americapriya_psalms100% (1)
- United States Complaint in Intervention in False Claims Act Lawsuits Accusing Insys Therapeutics of Paying Kickbacks and Engaging in Other Unlawful Practices to Promote Subsys, A Powerful Opioid PainkillerDocument37 pagesUnited States Complaint in Intervention in False Claims Act Lawsuits Accusing Insys Therapeutics of Paying Kickbacks and Engaging in Other Unlawful Practices to Promote Subsys, A Powerful Opioid PainkillerBeverly Tran100% (1)
- GSK Patient Assistance Program Application Check ListDocument5 pagesGSK Patient Assistance Program Application Check ListNerp FlimlotNo ratings yet
- Na PDP Classic Eoc 2022 Na2pdgeoc79428e RDocument146 pagesNa PDP Classic Eoc 2022 Na2pdgeoc79428e RMelva MosleyNo ratings yet
- Universal Engineering 2023 Benefit Guide FinalDocument53 pagesUniversal Engineering 2023 Benefit Guide Finaldanielduran003No ratings yet
- 2015 Winter DatelineDocument24 pages2015 Winter DatelineindydentalsocietyNo ratings yet
- Treat & Reduce Obesity ActDocument1 pageTreat & Reduce Obesity ActAubrey StuecklerNo ratings yet
- Part D PowerpointDocument14 pagesPart D PowerpointMark ReinhardtNo ratings yet
- Smileeee 86826468Document7 pagesSmileeee 86826468Frvrkpop LifeNo ratings yet
- California State Employees' Other Post Employment Benefits ReportDocument100 pagesCalifornia State Employees' Other Post Employment Benefits Reportjon_ortizNo ratings yet
- North Carolina and The Inflation Reduction ActDocument2 pagesNorth Carolina and The Inflation Reduction ActFOX8No ratings yet
- February 2021Document64 pagesFebruary 2021Eric SantiagoNo ratings yet
- HLOutlineDocument46 pagesHLOutlineCaylan HollandNo ratings yet
- 2012 U.S.Medicines Report PDFDocument56 pages2012 U.S.Medicines Report PDFRoberto Mosquera100% (1)
- Medicare Insurance Plans 2021 Is Expected To Start Enrolling in The Same Period As The Previous YearDocument3 pagesMedicare Insurance Plans 2021 Is Expected To Start Enrolling in The Same Period As The Previous YearInsureMeNowNo ratings yet
- Scope of Appointment FormDocument2 pagesScope of Appointment Formapi-260208821No ratings yet
- Account Field Reimbursement Manager in CA Resume Roger WortsmanDocument2 pagesAccount Field Reimbursement Manager in CA Resume Roger WortsmanRogerWortsmanNo ratings yet
- 2018-08-20 - OR4AD Comment To Task Force - Prices Paid by Oregonians - Rev2Document103 pages2018-08-20 - OR4AD Comment To Task Force - Prices Paid by Oregonians - Rev2Oregonians for Affordable Drug Prices NowNo ratings yet
- Redesigning For SpeedDocument11 pagesRedesigning For SpeedromainNo ratings yet