You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- PSYCHODYNAMICS AND JUDAISM The Jewish in Uences in Psychoanalysis and Psychodynamic TheoriesDocument33 pagesPSYCHODYNAMICS AND JUDAISM The Jewish in Uences in Psychoanalysis and Psychodynamic TheoriesCarla MissionaNo ratings yet
- Problem-Solution Essay Final DraftDocument4 pagesProblem-Solution Essay Final Draftapi-490864786No ratings yet
- Pediatric PoisoningDocument47 pagesPediatric PoisoningDr-Jagadeesh Mangamoori75% (4)
- Pediatric PoisoningDocument47 pagesPediatric PoisoningDr-Jagadeesh Mangamoori75% (4)
- Commercial LawDocument61 pagesCommercial LawthebfilesNo ratings yet
- Reaction PaperDocument3 pagesReaction PaperPatrick Ramos80% (15)
- Coaching Skills For Optimal PerformanceDocument58 pagesCoaching Skills For Optimal PerformanceYodhia Antariksa100% (3)
- ERP Test BankDocument29 pagesERP Test BankAsma 12No ratings yet
- Clinical PharmacyDocument60 pagesClinical PharmacyDr-Jagadeesh MangamooriNo ratings yet
- Medication AdherenceDocument36 pagesMedication AdherenceDr-Jagadeesh MangamooriNo ratings yet
- Robbins Ob14 PPT 11Document27 pagesRobbins Ob14 PPT 11daneshnedaieNo ratings yet
- Medication ErrorsDocument26 pagesMedication ErrorsDr-Jagadeesh Mangamoori75% (4)
- Gesture and Speech Andre Leroi-GourhanDocument451 pagesGesture and Speech Andre Leroi-GourhanFerda Nur Demirci100% (2)
- Planning Diets I1: How To Study 'I'His SectionDocument47 pagesPlanning Diets I1: How To Study 'I'His SectionDr-Jagadeesh MangamooriNo ratings yet
- Regional Meal Patterns: in ItDocument23 pagesRegional Meal Patterns: in ItDr-Jagadeesh MangamooriNo ratings yet
- Methods of Cooking: StudyDocument11 pagesMethods of Cooking: StudyDr-Jagadeesh MangamooriNo ratings yet
- Section 1 PDFDocument30 pagesSection 1 PDFSanjeev Kumar SinghNo ratings yet
- Finding Nutritive Value of Foodstuffs: How To Study This SectionDocument15 pagesFinding Nutritive Value of Foodstuffs: How To Study This SectionDr-Jagadeesh MangamooriNo ratings yet
- JCMSDocument6 pagesJCMSDr-Jagadeesh MangamooriNo ratings yet
- Finding Nutritive Value of Foodstuffs: How To Study This SectionDocument15 pagesFinding Nutritive Value of Foodstuffs: How To Study This SectionDr-Jagadeesh MangamooriNo ratings yet
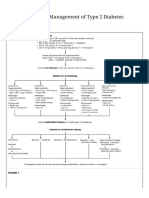
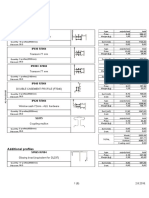
- Oral Agents in The Management of Type 2 Diabetes MellitusDocument2 pagesOral Agents in The Management of Type 2 Diabetes MellitusDr-Jagadeesh MangamooriNo ratings yet
- Pharm DDocument8 pagesPharm DDr-Jagadeesh MangamooriNo ratings yet
- Nutrition DefinitionDocument1 pageNutrition DefinitionDr-Jagadeesh MangamooriNo ratings yet
- Oral Agents in The Management of Type 2 Diabetes MellitusDocument2 pagesOral Agents in The Management of Type 2 Diabetes MellitusDr-Jagadeesh MangamooriNo ratings yet
- Nutrition and Food SystemsDocument1 pageNutrition and Food SystemsDr-Jagadeesh MangamooriNo ratings yet
- Novel CORONA Virus StructureDocument1 pageNovel CORONA Virus StructureDr-Jagadeesh MangamooriNo ratings yet
- IGNOU Common Prospectus EnglishDocument208 pagesIGNOU Common Prospectus Englishsanjibbhakta100% (1)
- One-Way Analysis of Variance For Independent or Correlated SamplesDocument4 pagesOne-Way Analysis of Variance For Independent or Correlated SamplesDr-Jagadeesh MangamooriNo ratings yet
- DNHE Program GuideDocument62 pagesDNHE Program GuideDr-Jagadeesh Mangamoori100% (1)
- Food Safety Officers Scheme Syllabus - APPSCDocument4 pagesFood Safety Officers Scheme Syllabus - APPSCDr-Jagadeesh MangamooriNo ratings yet
- NABH Hospitals ListDocument36 pagesNABH Hospitals ListDr-Jagadeesh MangamooriNo ratings yet
- IGNOU Common Prospectus EnglishDocument208 pagesIGNOU Common Prospectus Englishsanjibbhakta100% (1)
- Diagnosis of DKADocument1 pageDiagnosis of DKADr-Jagadeesh MangamooriNo ratings yet
- WHO - SchizophreniaDocument3 pagesWHO - SchizophreniaDr-Jagadeesh MangamooriNo ratings yet
- One-Way Analysis of Variance For Independent or Correlated SamplesDocument4 pagesOne-Way Analysis of Variance For Independent or Correlated SamplesDr-Jagadeesh MangamooriNo ratings yet
- Query: SWINE FLU-Definition, Causes, Signs and Symptoms, Management? ResponseDocument1 pageQuery: SWINE FLU-Definition, Causes, Signs and Symptoms, Management? ResponseDr-Jagadeesh MangamooriNo ratings yet
- Communication SkillsDocument70 pagesCommunication SkillsDr-Jagadeesh MangamooriNo ratings yet
- Lista Materijala WordDocument8 pagesLista Materijala WordAdis MacanovicNo ratings yet
- 2011 Physics B Form B Scoring GuidelinesDocument16 pages2011 Physics B Form B Scoring GuidelinesMichael CNo ratings yet
- Final Draft Basel II DissertationDocument110 pagesFinal Draft Basel II DissertationWilliam Weru80% (5)
- Computerized Dynamic Posturography (CDP)Document2 pagesComputerized Dynamic Posturography (CDP)eldescribdNo ratings yet
- mc96 97 01feb - PsDocument182 pagesmc96 97 01feb - PsMohammed Rizwan AliNo ratings yet
- Formulating A PICOT QuestionDocument4 pagesFormulating A PICOT QuestionKarl RobleNo ratings yet
- 145class 7 Integers CH 1Document2 pages145class 7 Integers CH 17A04Aditya MayankNo ratings yet
- Phonetic Sounds (Vowel Sounds and Consonant Sounds)Document48 pagesPhonetic Sounds (Vowel Sounds and Consonant Sounds)Jayson Donor Zabala100% (1)
- Radio Protection ChallengesDocument31 pagesRadio Protection ChallengesJackssonNo ratings yet
- Ebook PDF The Irony of Democracy An Uncommon Introduction To American Politics 17th Edition PDFDocument42 pagesEbook PDF The Irony of Democracy An Uncommon Introduction To American Politics 17th Edition PDFscott.stokley449100% (39)
- Incremental Analysis 2Document12 pagesIncremental Analysis 2enter_sas100% (1)
- Most Common Punctuation Errors Made English and Tefl Majors Najah National University - 0 PDFDocument24 pagesMost Common Punctuation Errors Made English and Tefl Majors Najah National University - 0 PDFDiawara MohamedNo ratings yet
- Jurnal Upload DR Selvi PDFDocument8 pagesJurnal Upload DR Selvi PDFRudi ChyprutNo ratings yet
- Recurrent: or Reinfection Susceptible People: Adult With Low Im Munity (Especially HIV Patient) Pathologic ChangesDocument36 pagesRecurrent: or Reinfection Susceptible People: Adult With Low Im Munity (Especially HIV Patient) Pathologic ChangesOsama SaidatNo ratings yet
- Agreement - AFS - RERA Punjab 20190906pro - Forma - Agreement - of - Sale - To - Be - Signed - With - AllotteesDocument35 pagesAgreement - AFS - RERA Punjab 20190906pro - Forma - Agreement - of - Sale - To - Be - Signed - With - AllotteesPuran Singh LabanaNo ratings yet
- Gamma Ray Interaction With Matter: A) Primary InteractionsDocument10 pagesGamma Ray Interaction With Matter: A) Primary InteractionsDr-naser MahmoudNo ratings yet
- Parathyroid Agents PDFDocument32 pagesParathyroid Agents PDFRhodee Kristine DoñaNo ratings yet
- HotsDocument74 pagesHotsgecko195No ratings yet
- City Living: Centro de Lenguas ExtranjerasDocument2 pagesCity Living: Centro de Lenguas Extranjerascolombia RodriguezNo ratings yet
- 002 Constraints and Generalized Coordinates PDFDocument27 pages002 Constraints and Generalized Coordinates PDFNiveCeciliaNo ratings yet
- Basic Foundation of Iv TherapyDocument10 pagesBasic Foundation of Iv Therapyjanna mae patriarcaNo ratings yet
- Experiment No 5 ZenerDocument3 pagesExperiment No 5 ZenerEugene Christina EuniceNo ratings yet