You might also like
- Csi Paper FinalDocument9 pagesCsi Paper Finalapi-337188982No ratings yet
- Pelvis LabDocument10 pagesPelvis Labapi-337188982No ratings yet
- Proknow Plan Study Report Head and Neck PlanDocument26 pagesProknow Plan Study Report Head and Neck Planapi-337188982No ratings yet
- Proknow Plan Study Report For Prone CsiDocument20 pagesProknow Plan Study Report For Prone Csiapi-337188982No ratings yet
- Combine Article AnalysisDocument14 pagesCombine Article Analysisapi-337188982No ratings yet
- Group 5-Mike Paul Charity Jessica FinalDocument13 pagesGroup 5-Mike Paul Charity Jessica Finalapi-332574751No ratings yet
- RT Submandibular Proknow CertificateDocument1 pageRT Submandibular Proknow Certificateapi-337188982No ratings yet
- Larynx Proknow CertificateDocument1 pageLarynx Proknow Certificateapi-337188982No ratings yet
- Qa Tables FinalDocument11 pagesQa Tables Finalapi-337188982No ratings yet
- Dos 711 Case Study FinalDocument15 pagesDos 711 Case Study Finalapi-337188982No ratings yet
- Lung Lab Final DraftDocument11 pagesLung Lab Final Draftapi-337188982No ratings yet
- Dos 516 Week 2 Paper Radiation SafetyDocument4 pagesDos 516 Week 2 Paper Radiation Safetyapi-337188982No ratings yet
- Dos 522 Attenuation Factor PaperDocument8 pagesDos 522 Attenuation Factor Paperapi-337188982No ratings yet
- Dos 531 Proknow CertificatesDocument3 pagesDos 531 Proknow Certificatesapi-337188982No ratings yet
- Dos 522 Head and Neck AssignmentDocument6 pagesDos 522 Head and Neck Assignmentapi-337188982No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Proposal Semister ProjectDocument7 pagesProposal Semister ProjectMuket AgmasNo ratings yet
- KSRTC BokingDocument2 pagesKSRTC BokingyogeshNo ratings yet
- Lista Precio Septiembre 0609Document75 pagesLista Precio Septiembre 0609gNo ratings yet
- Fundamental of Investment Unit 5Document8 pagesFundamental of Investment Unit 5commers bengali ajNo ratings yet
- Case Study - Soren ChemicalDocument3 pagesCase Study - Soren ChemicalSallySakhvadzeNo ratings yet
- Weibull Statistic and Growth Analysis in Failure PredictionsDocument9 pagesWeibull Statistic and Growth Analysis in Failure PredictionsgmitsutaNo ratings yet
- Guidelines On Accreditation of CSOs (LSB Representation) - DILG MC 2019-72Document18 pagesGuidelines On Accreditation of CSOs (LSB Representation) - DILG MC 2019-72Cedric Dequito100% (1)
- POS CAL SF No4 B2 BCF H300x300 7mmweld R0 PDFDocument23 pagesPOS CAL SF No4 B2 BCF H300x300 7mmweld R0 PDFNguyễn Duy QuangNo ratings yet
- Inflatable Packers enDocument51 pagesInflatable Packers enDavid LuhetoNo ratings yet
- AHP for Car SelectionDocument41 pagesAHP for Car SelectionNguyên BùiNo ratings yet
- Make a Battery Level Indicator using LM339 ICDocument13 pagesMake a Battery Level Indicator using LM339 ICnelson100% (1)
- Peter Wilkinson CV 1Document3 pagesPeter Wilkinson CV 1larry3108No ratings yet
- Instrumentos de Medición y Herramientas de Precisión Starrett DIAl TEST INDICATOR 196 A1ZDocument24 pagesInstrumentos de Medición y Herramientas de Precisión Starrett DIAl TEST INDICATOR 196 A1Zmicmarley2012No ratings yet
- Lec - Ray Theory TransmissionDocument27 pagesLec - Ray Theory TransmissionmathewNo ratings yet
- Customer Satisfaction and Brand Loyalty in Big BasketDocument73 pagesCustomer Satisfaction and Brand Loyalty in Big BasketUpadhayayAnkurNo ratings yet
- Entrepreneurship Style - MakerDocument1 pageEntrepreneurship Style - Makerhemanthreddy33% (3)
- Take Private Profit Out of Medicine: Bethune Calls for Socialized HealthcareDocument5 pagesTake Private Profit Out of Medicine: Bethune Calls for Socialized HealthcareDoroteo Jose Station100% (1)
- Asian Construction Dispute Denied ReviewDocument2 pagesAsian Construction Dispute Denied ReviewJay jogs100% (2)
- Erp and Mis Project - Thanks To PsoDocument31 pagesErp and Mis Project - Thanks To PsoAkbar Syed100% (1)
- Empowerment Technologies Learning ActivitiesDocument7 pagesEmpowerment Technologies Learning ActivitiesedzNo ratings yet
- SE Myth of SoftwareDocument3 pagesSE Myth of SoftwarePrakash PaudelNo ratings yet
- Backup and Recovery ScenariosDocument8 pagesBackup and Recovery ScenariosAmit JhaNo ratings yet
- Circular 09/2014 (ISM) : SubjectDocument7 pagesCircular 09/2014 (ISM) : SubjectDenise AhrendNo ratings yet
- Fundamentals of Marketing NotebookDocument24 pagesFundamentals of Marketing NotebookMorrisa AlexanderNo ratings yet
- Cib DC22692Document16 pagesCib DC22692Ashutosh SharmaNo ratings yet
- Indian Institute of Management KozhikodeDocument5 pagesIndian Institute of Management KozhikodepranaliNo ratings yet
- Simplex Addressable Breakglass PDFDocument12 pagesSimplex Addressable Breakglass PDFNurrul Ahmad Hidayat100% (1)
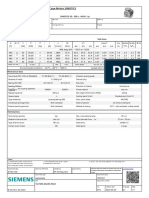
- 1LE1503-2AA43-4AA4 Datasheet enDocument1 page1LE1503-2AA43-4AA4 Datasheet enAndrei LupuNo ratings yet
- 1.1 Introduction To Networks - Networks Affect Our LivesDocument2 pages1.1 Introduction To Networks - Networks Affect Our LivesCristian MoralesNo ratings yet
- Hardened Concrete - Methods of Test: Indian StandardDocument16 pagesHardened Concrete - Methods of Test: Indian StandardjitendraNo ratings yet