You might also like
- Anaphy Patho BPHDocument5 pagesAnaphy Patho BPHRhea Mae Valles - ReyesNo ratings yet
- I Practiced The Following During Childbirth. 4 3 2 1 F WV WM QDDocument2 pagesI Practiced The Following During Childbirth. 4 3 2 1 F WV WM QDRhea Mae Valles - ReyesNo ratings yet
- Ms. Valles Wound Care Center: Submitted By: Rhea Mae V. Valles Bsn-Iii Submitted To: Mr. Ismael LagrasonDocument2 pagesMs. Valles Wound Care Center: Submitted By: Rhea Mae V. Valles Bsn-Iii Submitted To: Mr. Ismael LagrasonRhea Mae Valles - ReyesNo ratings yet
- Most Participative Most BehaveDocument4 pagesMost Participative Most BehaveRhea Mae Valles - ReyesNo ratings yet
- Case Analysis For Acute GastroenteritisDocument3 pagesCase Analysis For Acute GastroenteritisRhea Mae Valles - ReyesNo ratings yet
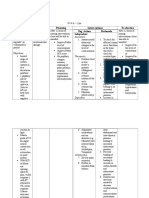
- Assessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleDocument2 pagesAssessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleRhea Mae Valles - ReyesNo ratings yet
- Ds Pedia WardDocument2 pagesDs Pedia WardRhea Mae Valles - ReyesNo ratings yet
- Assessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleDocument3 pagesAssessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleRhea Mae Valles - ReyesNo ratings yet
- Assessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleDocument4 pagesAssessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleRhea Mae Valles - ReyesNo ratings yet
- Drug Study: Rhea Mae V. Valles Bsn-IiiDocument1 pageDrug Study: Rhea Mae V. Valles Bsn-IiiRhea Mae Valles - ReyesNo ratings yet
- NCP Pt. GomezDocument2 pagesNCP Pt. GomezRhea Mae Valles - ReyesNo ratings yet
- Assessment Diagnosis Planning Intervention Evaluation Nsg. Action RationaleDocument3 pagesAssessment Diagnosis Planning Intervention Evaluation Nsg. Action RationaleRhea Mae Valles - ReyesNo ratings yet
- NCP Pt. DE ASISDocument3 pagesNCP Pt. DE ASISRhea Mae Valles - ReyesNo ratings yet
- Assessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleDocument3 pagesAssessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleRhea Mae Valles - ReyesNo ratings yet
- NCP Pt.Document3 pagesNCP Pt.Rhea Mae Valles - ReyesNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Paul FinanDocument35 pagesPaul FinanPinanto IrwandyNo ratings yet
- EAU Guidelines On: Penile CancerDocument38 pagesEAU Guidelines On: Penile Cancerhypebeast dopeNo ratings yet
- 28Document16 pages28Gus RamaNo ratings yet
- Small Animal OncologyDocument103 pagesSmall Animal Oncologyvet53No ratings yet
- Melanoma: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)Document154 pagesMelanoma: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)Ilham PermanaNo ratings yet
- Group 4 Thyroid Storm ALADocument25 pagesGroup 4 Thyroid Storm ALAJessica RamosNo ratings yet
- Vaccine HistoryDocument35 pagesVaccine HistoryEhed AymazNo ratings yet
- Molecular Mechanism of Cancer MetastasisDocument43 pagesMolecular Mechanism of Cancer MetastasisDipesh Ludhwani100% (1)
- Periampullary Carcinoma - Surgical Treatment - NCBI Bookshelf PDFDocument4 pagesPeriampullary Carcinoma - Surgical Treatment - NCBI Bookshelf PDFAsif.N.IqbalNo ratings yet
- Principles of OncologyDocument26 pagesPrinciples of OncologyDr Shahzad Alam ShahNo ratings yet
- Current Concepts in Plastic Surgery - AgulloDocument273 pagesCurrent Concepts in Plastic Surgery - AgulloAnonymous LnWIBo1GNo ratings yet
- Hilar EnlargementDocument19 pagesHilar EnlargementGriggrogGingerNo ratings yet
- Articol Medicina de TrimisDocument19 pagesArticol Medicina de TrimisMoldovan TiberiuNo ratings yet
- Biomarkers Diagnostic ProgramDocument23 pagesBiomarkers Diagnostic ProgramAndraReiNo ratings yet
- Cross Trial - Preoperative Chemoradiotherapy For Esophageal or Junctional Cancer - Nejm 2012Document12 pagesCross Trial - Preoperative Chemoradiotherapy For Esophageal or Junctional Cancer - Nejm 2012api-308365861No ratings yet
- Nasopharyngeal CARCINOMADocument37 pagesNasopharyngeal CARCINOMAAdrian Prasetya SudjonoNo ratings yet
- Recent Advances in The Management of LiposarcomaDocument15 pagesRecent Advances in The Management of LiposarcomaBudhiNo ratings yet
- Raf Kinase Inhibitor Protein PositivelyDocument14 pagesRaf Kinase Inhibitor Protein PositivelyGabriel FenteanyNo ratings yet
- Advances in Prostate Cancer - G. Hamilton (Intech, 2013) WW PDFDocument700 pagesAdvances in Prostate Cancer - G. Hamilton (Intech, 2013) WW PDFdvisionNo ratings yet
- Embryology and Functional Anatomy of The BreastDocument20 pagesEmbryology and Functional Anatomy of The BreastseidkeNo ratings yet
- Surgical ConditionsDocument116 pagesSurgical ConditionsFan EliNo ratings yet
- Oncology Lectures 1 7 DR - FerrolinoDocument24 pagesOncology Lectures 1 7 DR - FerrolinoMiguel Cuevas DolotNo ratings yet
- Radiofrequency Ablation: Technique and Clinical ApplicationsDocument10 pagesRadiofrequency Ablation: Technique and Clinical ApplicationsAbhi RajNo ratings yet
- German Hyperthermia ClinicsDocument91 pagesGerman Hyperthermia ClinicsPrabhjot SinghNo ratings yet
- Grossing Technique in BreastDocument37 pagesGrossing Technique in BreastadiNo ratings yet
- 08 Pathology Orthobullets2017 PDFDocument189 pages08 Pathology Orthobullets2017 PDFdr_shafiq100% (1)
- Class 6 PathologyDocument4 pagesClass 6 PathologyMostafizur RahmanNo ratings yet
- Care of Clients With Cellular Aberrations: NCM 106/ NCM 112Document22 pagesCare of Clients With Cellular Aberrations: NCM 106/ NCM 112Janelle Cabida SupnadNo ratings yet
- Lung Cancer Literature ReviewDocument4 pagesLung Cancer Literature Reviewc5qwqy8v100% (1)
- All Information Is On Websit:: Soft Tissue Tumours by Dr. Fahd Al-MullaDocument45 pagesAll Information Is On Websit:: Soft Tissue Tumours by Dr. Fahd Al-Mullariskhapangestika100% (1)