You might also like
- Flunarizine Effective Migrainous Vertigo PreventionDocument6 pagesFlunarizine Effective Migrainous Vertigo PreventionNanda WtNo ratings yet
- Oxygen For Cluster Headaches: A GuideDocument25 pagesOxygen For Cluster Headaches: A GuidetriaclaresiaNo ratings yet
- Creamer Et Al-2016-British Journal of DermatologyDocument34 pagesCreamer Et Al-2016-British Journal of DermatologyAtika Indah SariNo ratings yet
- Initial Severity of Schizophrenia and EfficacyDocument20 pagesInitial Severity of Schizophrenia and EfficacytriaclaresiaNo ratings yet
- Tugas Ekspertise AbdomenDocument42 pagesTugas Ekspertise AbdomentriaclaresiaNo ratings yet
- Perioperative Dextromethorphan As An Adjunct For Postoperative PainDocument10 pagesPerioperative Dextromethorphan As An Adjunct For Postoperative PaintriaclaresiaNo ratings yet
- A Comparative Effectiveness Meta-Analysis of Drugs For The Prophylaxis of Migraine HeadacheDocument60 pagesA Comparative Effectiveness Meta-Analysis of Drugs For The Prophylaxis of Migraine HeadachetriaclaresiaNo ratings yet
- De-Regil Et Al-2016-The Cochrane LibraryDocument124 pagesDe-Regil Et Al-2016-The Cochrane LibrarytriaclaresiaNo ratings yet
- E. HystoliticaDocument7 pagesE. HystoliticatriaclaresiaNo ratings yet
- Yoi 140088Document779 pagesYoi 140088triaclaresiaNo ratings yet
- Clinical Use of BloodDocument221 pagesClinical Use of BloodRizma Adlia100% (1)
- Guidelines For The Administration of Blood and Blood ComponentsDocument29 pagesGuidelines For The Administration of Blood and Blood ComponentsCindya PerthyNo ratings yet
- Benign Paroxysmal Positional VertigoDocument65 pagesBenign Paroxysmal Positional VertigoReni SusantiNo ratings yet
- Panss ScoreDocument8 pagesPanss ScoretriaclaresiaNo ratings yet
- BPPVDocument36 pagesBPPVRizka AmaliaNo ratings yet
- MeniereDocument50 pagesMenieretriaclaresiaNo ratings yet
- S1 Diet, Immune and InfectionDocument48 pagesS1 Diet, Immune and InfectiontriaclaresiaNo ratings yet
- Introduction To Serology - Immunology, HSV & H.pyloriDocument37 pagesIntroduction To Serology - Immunology, HSV & H.pyloritriaclaresiaNo ratings yet
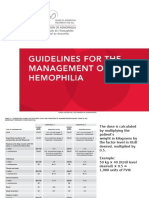
- Dosis HemofiliaDocument5 pagesDosis HemofiliatriaclaresiaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Physically IncorrectDocument524 pagesPhysically IncorrectdrumsetmanNo ratings yet
- Biology A (Salters Nuffield) : Pearson Edexcel Level 3 GCEDocument36 pagesBiology A (Salters Nuffield) : Pearson Edexcel Level 3 GCEGershonNo ratings yet
- Class 3 Dps Evs Enrichment 2019Document3 pagesClass 3 Dps Evs Enrichment 2019ArchanaGuptaNo ratings yet
- Journal of Pregnancy and Child Health Article 1 PDFDocument3 pagesJournal of Pregnancy and Child Health Article 1 PDFNeha MishraNo ratings yet
- Nutrition AssessmentDocument32 pagesNutrition AssessmentJobelyn MalisaNo ratings yet
- Kettlebell Training GuideDocument16 pagesKettlebell Training GuideGöran Svensson100% (3)
- Recovery and Regeneration For Basketball PlayersDocument19 pagesRecovery and Regeneration For Basketball PlayerseretriaNo ratings yet
- International Journal Health Research: of of of ofDocument10 pagesInternational Journal Health Research: of of of ofnewewi333No ratings yet
- Mars On 2016Document27 pagesMars On 2016Lucss TrigoNo ratings yet
- Types of Fats: Saturated, Unsaturated, TransDocument2 pagesTypes of Fats: Saturated, Unsaturated, TransMarie Antionette MondragonNo ratings yet
- Management Nutrisi Pada Stroke Akut DR Mursyid FinalDocument31 pagesManagement Nutrisi Pada Stroke Akut DR Mursyid Finalkanes eisaNo ratings yet
- Obesity Case StudyDocument10 pagesObesity Case StudyPhavarasan ArasanNo ratings yet
- Childhood Obesity ProgramsDocument28 pagesChildhood Obesity ProgramsWan Azlan Wan HalimNo ratings yet
- Dds-Glucose GOD 10 Min.Document2 pagesDds-Glucose GOD 10 Min.Eureka SevenNo ratings yet
- Daftar Pustaka Diabetes MellitusDocument4 pagesDaftar Pustaka Diabetes MellitusHanderson Varalta100% (1)
- What Is Malnutrition?: WastingDocument6 pagesWhat Is Malnutrition?: WastingĐoan VõNo ratings yet
- Dressage Rider Fitness TrainingDocument23 pagesDressage Rider Fitness Trainingapi-497348165100% (1)
- Pregnancy Induced Hypertension Case StudyDocument54 pagesPregnancy Induced Hypertension Case Studysupernurse02No ratings yet
- B-MIDTERMS EXAM-NutriLECDocument7 pagesB-MIDTERMS EXAM-NutriLECNelia AlfonsoNo ratings yet
- German Volume Training Mutliple Routines - Use This OneDocument6 pagesGerman Volume Training Mutliple Routines - Use This OneJohn Smith100% (1)
- MedicineDocument48 pagesMedicineKasun Perera0% (1)
- Strategic Issue - Obesity - Health Living v2Document2 pagesStrategic Issue - Obesity - Health Living v2vqw6No ratings yet
- 21 Day Boulder ShouldersDocument8 pages21 Day Boulder Shouldersfdndrd0% (1)
- UOE With Open Cloze and Multiple Choice and TensesDocument2 pagesUOE With Open Cloze and Multiple Choice and Tensesmalenatobe100% (1)
- The Belly Fat Diet John ChathamDocument92 pagesThe Belly Fat Diet John ChathamGurpreet Kaur100% (3)
- Bodybuilding NutritionDocument11 pagesBodybuilding NutritionFirmansyah Tri Saputra100% (1)
- ELDERLY HEALTH CARE IN ILIGAN CITYDocument27 pagesELDERLY HEALTH CARE IN ILIGAN CITYKristelle Sultero PaniamoganNo ratings yet
- Effects of Low Versus High Volume High Intensity Interval - 2023 - Journal of EDocument10 pagesEffects of Low Versus High Volume High Intensity Interval - 2023 - Journal of ESherriNo ratings yet
- ANC-1 ASSIGNMENT 1: NUTRITION FOR THE COMMUNITYDocument6 pagesANC-1 ASSIGNMENT 1: NUTRITION FOR THE COMMUNITYprinceforjesus0% (1)
- Total Hip Replacement Patient GuidelinesDocument44 pagesTotal Hip Replacement Patient GuidelinesDr-Mudassar Ali PTNo ratings yet