You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Drug of Abuse (Table) PDFDocument2 pagesDrug of Abuse (Table) PDFtchanochNo ratings yet
- Chapter 1 Introduction To Emergency Medical CareDocument19 pagesChapter 1 Introduction To Emergency Medical Carejmmos207064100% (1)
- CPR Study Guide 2021: Online CPR Cheat SheetDocument14 pagesCPR Study Guide 2021: Online CPR Cheat SheetHenz Freeman0% (1)
- טיפול ב חוסרהשקט חדDocument2 pagesטיפול ב חוסרהשקט חדtchanochNo ratings yet
- 63 Must Know Lab Values Cheat Sheet - NCLEX (Caribbean Nurses of Puerto Rico and Latin America) PDFDocument4 pages63 Must Know Lab Values Cheat Sheet - NCLEX (Caribbean Nurses of Puerto Rico and Latin America) PDFChristineBiankii100% (1)
- Treatment of Acute Agitation in Psychotic Disorders PDFDocument9 pagesTreatment of Acute Agitation in Psychotic Disorders PDFtchanochNo ratings yet
- 10 Common EKG Heart Rhythms PDFDocument1 page10 Common EKG Heart Rhythms PDFtchanochNo ratings yet
- IMLE Flash Cards AlmosadoctorDocument33 pagesIMLE Flash Cards Almosadoctortchanoch100% (1)
- H B PoemDocument1 pageH B PoemtchanochNo ratings yet
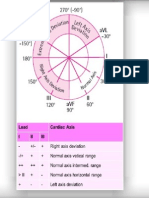
- Ecg Axis DeviationDocument1 pageEcg Axis DeviationtchanochNo ratings yet
- Ecg AxisDocument1 pageEcg AxistchanochNo ratings yet
- Ecg TopoDocument1 pageEcg TopotchanochNo ratings yet
- Drug of Abuse (Table) B PDFDocument2 pagesDrug of Abuse (Table) B PDFtchanochNo ratings yet
- שחזור מרץ 2012Document31 pagesשחזור מרץ 2012tchanoch0% (1)
- Postmortem Biochemistry of Vitreous Humor and Glucose MetabolismDocument7 pagesPostmortem Biochemistry of Vitreous Humor and Glucose MetabolismsbeyeforhireNo ratings yet
- Role of MDCT in Coronary Artery Disease: Swachchhanda Songmen 2071Document63 pagesRole of MDCT in Coronary Artery Disease: Swachchhanda Songmen 2071Dr KhanNo ratings yet
- Orthopedic NursingDocument201 pagesOrthopedic NursingMitch Hellgirl Almonte100% (2)
- Pre - Operative SurgeryDocument3 pagesPre - Operative SurgeryFan Eli100% (5)
- Tracheostomy Site CancerDocument2 pagesTracheostomy Site CancerСварооп СатурнскыNo ratings yet
- Controversies in Condylar Fracture Repair UntalanDocument35 pagesControversies in Condylar Fracture Repair UntalanFrederick Mars Untalan100% (1)
- Prevention of Ebola Virus InfectionDocument55 pagesPrevention of Ebola Virus InfectionAnusha VergheseNo ratings yet
- Diabetes Care in Nigeria - 2015 - Annals of Global Health PDFDocument9 pagesDiabetes Care in Nigeria - 2015 - Annals of Global Health PDFarmanNo ratings yet
- Clinical Experience With Surgical Debridement and Simultaneous Meshed Skin Grafts in Treating Biofilm-Associated Infection: An Exploratory Retrospective Pilot StudyDocument9 pagesClinical Experience With Surgical Debridement and Simultaneous Meshed Skin Grafts in Treating Biofilm-Associated Infection: An Exploratory Retrospective Pilot StudyAsmat BurhanNo ratings yet
- Lugols Solution Schillers Test IFU V9 EN4Document1 pageLugols Solution Schillers Test IFU V9 EN4Mary's CatzNo ratings yet
- Acute Stress Disorder 1Document22 pagesAcute Stress Disorder 1Seiska MegaNo ratings yet
- Principles & Practice of First AidDocument298 pagesPrinciples & Practice of First AidJoshua100% (2)
- Tingkat Kepatuhan Antihipertensi Dan Pengontrolan Tekanan Darah Pasien Rawat Jalan Rs Pku Muhammadiyah BantulDocument6 pagesTingkat Kepatuhan Antihipertensi Dan Pengontrolan Tekanan Darah Pasien Rawat Jalan Rs Pku Muhammadiyah BantulRusnaneeNo ratings yet
- PG - 2016 - 2017 SESSION List of Candidates Allotted - On 11.04.2016Document16 pagesPG - 2016 - 2017 SESSION List of Candidates Allotted - On 11.04.2016chenda raviNo ratings yet
- Mock SurgeryDocument7 pagesMock SurgeryElegant Dental clinicNo ratings yet
- Complete Ophtho VM555 CoursepackDocument189 pagesComplete Ophtho VM555 Coursepacknandhus2227No ratings yet
- Viral ConjunctivitisDocument15 pagesViral ConjunctivitisMary Cathlane TeroNo ratings yet
- Antuñano 2000 PDFDocument10 pagesAntuñano 2000 PDFAlonso FlNo ratings yet
- Template MRDocument27 pagesTemplate MRdipo buyerNo ratings yet
- Water Birth PPDocument5 pagesWater Birth PPAzi SamiNo ratings yet
- GC-#1580121-V1-Naphcare #70624-23 Inmate Health Care Services AgreementDocument110 pagesGC-#1580121-V1-Naphcare #70624-23 Inmate Health Care Services AgreementActionNewsJaxNo ratings yet
- TransplantDocument30 pagesTransplantLoshi ChandrasekarNo ratings yet
- Managing Adult Insomnia ConfidentlyDocument8 pagesManaging Adult Insomnia ConfidentlyJuliana RodriguezNo ratings yet
- Sarhad 8MCF BadlmaDocument29 pagesSarhad 8MCF Badlmasoran najebNo ratings yet
- Essay On Fracture ComplicationsDocument9 pagesEssay On Fracture ComplicationsadibahNo ratings yet
- JFMPC 9 526Document5 pagesJFMPC 9 526nadiancupNo ratings yet
- Pembrolizumab For The Treatment of Cervical CancerDocument31 pagesPembrolizumab For The Treatment of Cervical CancerluizaNo ratings yet
- Sas 20Document4 pagesSas 20Sistine Rose LabajoNo ratings yet