You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Sin Título 42Document9 pagesSin Título 42Charles JacksonNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hyper Boom Portfolio - wbt856Document28 pagesThe Hyper Boom Portfolio - wbt856Charles Jackson100% (5)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- 18 Hofmann & Hayes (In Press) The Future of Intervention Science - Process Based TherapyDocument41 pages18 Hofmann & Hayes (In Press) The Future of Intervention Science - Process Based TherapyCharles JacksonNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- 11 Holzel Et Al 2011 - How MFN WorksDocument24 pages11 Holzel Et Al 2011 - How MFN WorksCharles JacksonNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- McCallin, A. (2001) - Interdisciplinary Practice-A Matter of TeamworkDocument10 pagesMcCallin, A. (2001) - Interdisciplinary Practice-A Matter of TeamworkCharles JacksonNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Concept Analysis of Interdisciplinary PDFDocument11 pagesConcept Analysis of Interdisciplinary PDFCharles JacksonNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Ryder, A.G., Costa, P.T., JR., & Bagby, R. M. (2007)Document12 pagesRyder, A.G., Costa, P.T., JR., & Bagby, R. M. (2007)AnaerobiosNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
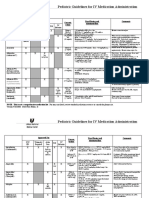
- Pediatric Guidelines For MedicationsDocument24 pagesPediatric Guidelines For MedicationsjonatasmartinezNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- ScoreDocument43 pagesScorepokharelriwaj82No ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Terapi Bekam Dalam Menurunkan Intensitas Dismenore Dan Tanda-Tanda Vital (Nadi Dan Tekanan Darah)Document8 pagesTerapi Bekam Dalam Menurunkan Intensitas Dismenore Dan Tanda-Tanda Vital (Nadi Dan Tekanan Darah)Milkha AmaliaNo ratings yet
- 6 Hypertension Nursing Care - Arif Setyo UpoyoDocument40 pages6 Hypertension Nursing Care - Arif Setyo UpoyoRizka Nur AgustinNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Approach To Acutely Ill PatientDocument22 pagesApproach To Acutely Ill PatientSarah RamliNo ratings yet
- Comprehensive Hesi Review 1Document68 pagesComprehensive Hesi Review 1Tamara Smith-Williams100% (26)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Mantle TceDocument8 pagesMantle TceNoe Rodriguez DiazNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- 1 s2.0 S0895435615000141 MainDocument10 pages1 s2.0 S0895435615000141 MainBarron ManNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Appendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexDocument26 pagesAppendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexabigailNo ratings yet
- Medical Diseases in PregnancyDocument37 pagesMedical Diseases in PregnancyAsteway MesfinNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Class X CH-6 WS Answer KeyDocument6 pagesClass X CH-6 WS Answer KeyYASHVI MODINo ratings yet
- Acute Compartment Syndrome of The Extremities - UpToDateDocument22 pagesAcute Compartment Syndrome of The Extremities - UpToDateSatrio Bangun NegoroNo ratings yet
- Drug Study: Valerie V. Villanueva BN3-CDocument2 pagesDrug Study: Valerie V. Villanueva BN3-CA.No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 409 Pope, B. and Maillie, S. CCRN-PCCN Review Multisystem and Q and ADocument21 pages409 Pope, B. and Maillie, S. CCRN-PCCN Review Multisystem and Q and Agliftan100% (2)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Prevalence of Diabetic Retinopathy and Its Associated Factors Among Diabetic Patients at Debre Markos Referral Hospital, Northwest Ethiopia, 2019: Hospital-Based Cross-Sectional StudyDocument9 pagesPrevalence of Diabetic Retinopathy and Its Associated Factors Among Diabetic Patients at Debre Markos Referral Hospital, Northwest Ethiopia, 2019: Hospital-Based Cross-Sectional StudyVivi DeviyanaNo ratings yet
- NCP PreeclampsiaDocument2 pagesNCP Preeclampsiasteffi100% (1)
- HHDocument9 pagesHHzainul umariNo ratings yet
- Mennen Envoy GGHDocument612 pagesMennen Envoy GGHEva TelloNo ratings yet
- Unit 1 Concepts of Physical FitnessDocument116 pagesUnit 1 Concepts of Physical FitnessnanaNo ratings yet
- B105 Patient Monitor: Care With ConfidenceDocument5 pagesB105 Patient Monitor: Care With ConfidenceNoe Muñoz QuitoNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Electrocardiographic Criteria For The Diagnosis of Left Ventricular HypertrophyDocument10 pagesElectrocardiographic Criteria For The Diagnosis of Left Ventricular HypertrophyHendri SaputraNo ratings yet
- Initial Assessment and Management of Acute StrokeDocument49 pagesInitial Assessment and Management of Acute StrokeIrina DuceacNo ratings yet
- Online Anatomy and Physiology Lab ManualDocument37 pagesOnline Anatomy and Physiology Lab ManualcalagorubilanceNo ratings yet
- Effects of PneumoperitoneumDocument30 pagesEffects of PneumoperitoneumRajarshi KumarNo ratings yet
- Laerdal SimPad BrochureDocument7 pagesLaerdal SimPad BrochureEnerspect Medical SolutionsNo ratings yet
- Mechanism of Propranolol Withdrawal PhenomenaDocument7 pagesMechanism of Propranolol Withdrawal PhenomenaAsmaa LabibNo ratings yet
- Knowledge, Attitude and Practice On Hypertension Among Antihypertensive Medication UsersDocument7 pagesKnowledge, Attitude and Practice On Hypertension Among Antihypertensive Medication UsersMuhammad DeddyNo ratings yet
- Zoll M-Series NIBP CalibrationDocument34 pagesZoll M-Series NIBP CalibrationChris SilerNo ratings yet
- H. Pathophysiology I. Definition of Diagnosis A) Pregnancy Induced HypertensionDocument9 pagesH. Pathophysiology I. Definition of Diagnosis A) Pregnancy Induced HypertensionEmmy Flor ValmoriaNo ratings yet
- POCUS Sobrecarga 2022Document13 pagesPOCUS Sobrecarga 2022tavo570No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)