You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- RegexDocument1 pageRegexNzNo ratings yet
- Semi-Supervised Classification With Graph Convolutional NetworksDocument14 pagesSemi-Supervised Classification With Graph Convolutional NetworksZafarNo ratings yet
- Granulocyte-Colony Stimulating Factor Promotes Lung Metastasis Through Mobilization of Ly6G+Ly6C+ GranulocytesDocument8 pagesGranulocyte-Colony Stimulating Factor Promotes Lung Metastasis Through Mobilization of Ly6G+Ly6C+ GranulocytesSaiful IslamNo ratings yet
- rnn-1406 1078 PDFDocument15 pagesrnn-1406 1078 PDFalanNo ratings yet
- Guideline For Good Evaluation Practice in Health Informatics (GEP-HI)Document13 pagesGuideline For Good Evaluation Practice in Health Informatics (GEP-HI)Saiful IslamNo ratings yet
- Img 20180307 0001 2Document2 pagesImg 20180307 0001 2Saiful IslamNo ratings yet
- C EssentialsDocument45 pagesC EssentialssuchitraprasannaNo ratings yet
- Neural Machine Translation PDFDocument15 pagesNeural Machine Translation PDFAkash GuptaNo ratings yet
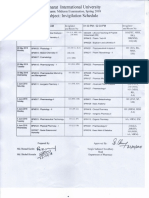
- Invigilation Schedule of Spring 2018Document1 pageInvigilation Schedule of Spring 2018Saiful IslamNo ratings yet
- FullDocument20 pagesFullSaiful IslamNo ratings yet
- Sa - Vocabulary ListDocument61 pagesSa - Vocabulary ListSaiful IslamNo ratings yet
- Get Started With Dropbox PDFDocument10 pagesGet Started With Dropbox PDFANo ratings yet
- Quiz LetDocument135 pagesQuiz LetSaiful IslamNo ratings yet
- In Liner Notes,' Loudon Wainwright Looks Squarely at His Flaws and His Musical Family Tree - The New York TimesDocument4 pagesIn Liner Notes,' Loudon Wainwright Looks Squarely at His Flaws and His Musical Family Tree - The New York TimesSaiful IslamNo ratings yet
- Solved Problem in ProbabilityDocument3 pagesSolved Problem in ProbabilitySaiful IslamNo ratings yet
- Introduction To Linear Algebra: (4th Edition)Document3 pagesIntroduction To Linear Algebra: (4th Edition)Saiful IslamNo ratings yet
- RibaDocument3 pagesRibaSaiful IslamNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- NCP EpilepsyDocument1 pageNCP EpilepsyManpreet ToorNo ratings yet
- Sensory Analysis v2 2Document16 pagesSensory Analysis v2 2Alyssa BalverdeNo ratings yet
- Cardio NclexDocument40 pagesCardio NclexGabrielle WashingtonNo ratings yet
- Health Drama: To Meet One of The Tasks English Course Lecturer: Deny Abdillah M, M.PDDocument6 pagesHealth Drama: To Meet One of The Tasks English Course Lecturer: Deny Abdillah M, M.PDnadia hanifaNo ratings yet
- Myocardial Infarct Checklist: TIMELINE // DateDocument2 pagesMyocardial Infarct Checklist: TIMELINE // DateMohd Syamirulah RahimNo ratings yet
- AAO 2015 Instruction Course (Mystery Retina-Interactive Discussion of Cases) - Final HandoutDocument45 pagesAAO 2015 Instruction Course (Mystery Retina-Interactive Discussion of Cases) - Final HandoutJennifer Kang-MielerNo ratings yet
- NEJM GoutDocument9 pagesNEJM GoutAnonymous G26HIUtzV100% (1)
- PTSD EssayDocument2 pagesPTSD Essayapi-335023853No ratings yet
- Critical Care Infection ControlDocument41 pagesCritical Care Infection ControlMisbah 114No ratings yet
- Cup of Kindness: NHS Greater Glasgow and ClydeDocument16 pagesCup of Kindness: NHS Greater Glasgow and ClydecrispypataNo ratings yet
- Advocacy PaperDocument3 pagesAdvocacy Paperapi-485309966No ratings yet
- Geriatric AssessmentDocument2 pagesGeriatric AssessmentAzubuike Ifejoku-ChukwukaNo ratings yet
- M2S3Document12 pagesM2S3Jeson EtormaNo ratings yet
- Assignment 1 FinalDocument5 pagesAssignment 1 Finalapi-316011285No ratings yet
- Schenke in 2006Document17 pagesSchenke in 2006Rest0No ratings yet
- The ShelfDocument18 pagesThe Shelfsowcowdd100% (5)
- Newport, D.J. and Nemeroff, C.B. Neurobiology of Posttraumatic Stress Disorder. Cognitive Neuroscience JAARTALDocument8 pagesNewport, D.J. and Nemeroff, C.B. Neurobiology of Posttraumatic Stress Disorder. Cognitive Neuroscience JAARTALg10564433No ratings yet
- EcgDocument10 pagesEcgKarthik ManoharanNo ratings yet
- Legalizing MarijuanaDocument3 pagesLegalizing MarijuanaAlyssa MabalotNo ratings yet
- Traditional Filipino healing practices and beliefsDocument70 pagesTraditional Filipino healing practices and beliefsJennifer BolongNo ratings yet
- Trauma and Spine Sessions at Medical ConferenceDocument5 pagesTrauma and Spine Sessions at Medical ConferencesrisaravananNo ratings yet
- Legal Med FinalDocument59 pagesLegal Med FinalCriminology Criminology CriminologyNo ratings yet
- MaprotilineDocument10 pagesMaprotilineAnonymous U4E6I1R100% (1)
- Tamsulosin Hydro ChlorideDocument2 pagesTamsulosin Hydro Chlorideapi-3797941100% (3)
- Apollo Hospital Management System SRSDocument14 pagesApollo Hospital Management System SRSVishwa Sourab Brungi100% (2)
- G 098 DatasetforthyroidcancerhistopathologyreportsfinalDocument21 pagesG 098 DatasetforthyroidcancerhistopathologyreportsfinalCarloscharlieranaNo ratings yet
- Neurogenic Bladder: When Nerve Damage Causes Bladder ProblemsDocument3 pagesNeurogenic Bladder: When Nerve Damage Causes Bladder ProblemsmarselamgeNo ratings yet
- Gallstones: Causes, Symptoms and TreatmentDocument15 pagesGallstones: Causes, Symptoms and Treatmenthisabumohamed100% (1)
- Courier WedgeDocument19 pagesCourier WedgesurfnewmediaNo ratings yet
- Using Intraoral Gothic Arch Tracing To Balance Full Dentures and Determine Centric Relation and Occlusal Vertical DimensionDocument15 pagesUsing Intraoral Gothic Arch Tracing To Balance Full Dentures and Determine Centric Relation and Occlusal Vertical DimensionAlfred OrozcoNo ratings yet