You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- John Deere 772d 6wd GraderDocument6 pagesJohn Deere 772d 6wd GraderyaserattiaNo ratings yet
- Introduction To Probability: Business Statistics: Communicating With Numbers, 4eDocument52 pagesIntroduction To Probability: Business Statistics: Communicating With Numbers, 4eRetno Ajeng Anissa WidiatriNo ratings yet
- Novel Technique For Management of Bartholin Gland CystsnDocument3 pagesNovel Technique For Management of Bartholin Gland CystsnelenNo ratings yet
- Noc18 cs48 Assignment3Document4 pagesNoc18 cs48 Assignment3shweta100% (1)
- Leviton ManualDocument82 pagesLeviton ManualRobby Larson100% (1)
- Adrenal Androgen Excess and Body Mass Index in PCOSDocument9 pagesAdrenal Androgen Excess and Body Mass Index in PCOSelenNo ratings yet
- Thyroid Autoimmunity and Female Infertility: Kris Poppe, Daniel Glinoer, Brigitte VelkeniersDocument16 pagesThyroid Autoimmunity and Female Infertility: Kris Poppe, Daniel Glinoer, Brigitte VelkenierselenNo ratings yet
- Gynecology and Minimally Invasive Therapy: Case ReportDocument5 pagesGynecology and Minimally Invasive Therapy: Case ReportelenNo ratings yet
- (DHEA) Replacement Decreases Insulin Resistance and Lower Inflamatory CytokineDocument10 pages(DHEA) Replacement Decreases Insulin Resistance and Lower Inflamatory CytokineelenNo ratings yet
- Stem Cells Ray of Hope in InfertilityDocument2 pagesStem Cells Ray of Hope in InfertilityelenNo ratings yet
- Drainage of Bartholin Cyst Abscess ML46071Document4 pagesDrainage of Bartholin Cyst Abscess ML46071elenNo ratings yet
- A Review Leptin Structure and Mechanism Actions"Document8 pagesA Review Leptin Structure and Mechanism Actions"elenNo ratings yet
- 03 Bartholin Gland Procedure + Inform ConsentDocument4 pages03 Bartholin Gland Procedure + Inform ConsentelenNo ratings yet
- Bartholin Cyst or Abscess - Leaflet v3 April 17Document2 pagesBartholin Cyst or Abscess - Leaflet v3 April 17elenNo ratings yet
- Bar Tho LinDocument6 pagesBar Tho LinArwin OkwandiNo ratings yet
- Causes of Infertility in Women at Reproductive Age PDFDocument8 pagesCauses of Infertility in Women at Reproductive Age PDFelenNo ratings yet
- Pid FaqDocument3 pagesPid FaqLili ManaoNo ratings yet
- Drainage of Bartholin Cyst Abscess ML46071Document4 pagesDrainage of Bartholin Cyst Abscess ML46071elenNo ratings yet
- Distribution of Infertility Factors Among Infertile Couples in YemenDocument4 pagesDistribution of Infertility Factors Among Infertile Couples in YemenelenNo ratings yet
- Diagnosis and Management of Graves' Disease: Review SynthèseDocument11 pagesDiagnosis and Management of Graves' Disease: Review Synthèsedanil armandNo ratings yet
- Comparison of Visual Inspection and Papanicolau (PAP) SmearsDocument8 pagesComparison of Visual Inspection and Papanicolau (PAP) SmearselenNo ratings yet
- Is There Any in Women Consulting Fertility TXDocument7 pagesIs There Any in Women Consulting Fertility TXelenNo ratings yet
- Clinical Impact of Postsurgical Adhesions1 PDFDocument10 pagesClinical Impact of Postsurgical Adhesions1 PDFTito AlhoNo ratings yet
- Cervical CancerDocument60 pagesCervical CancerNova Yuli PrasetyoNo ratings yet
- Thyroid Autoimmunity and Female Infertility: Kris Poppe, Daniel Glinoer, Brigitte VelkeniersDocument16 pagesThyroid Autoimmunity and Female Infertility: Kris Poppe, Daniel Glinoer, Brigitte VelkenierselenNo ratings yet
- Effect of A High-Fat Diet On 24-h Pattern of Circulating LevelsDocument8 pagesEffect of A High-Fat Diet On 24-h Pattern of Circulating LevelselenNo ratings yet
- Diagnostic Value of The Risk of Malignancy Index (RMI) For Detection of Pelvic Malignancies ComparedDocument6 pagesDiagnostic Value of The Risk of Malignancy Index (RMI) For Detection of Pelvic Malignancies ComparedelenNo ratings yet
- Enteral Nutrition Therapy For The Surgical PatientDocument52 pagesEnteral Nutrition Therapy For The Surgical PatientelenNo ratings yet
- Clinical Impact of Postsurgical Adhesions1 PDFDocument10 pagesClinical Impact of Postsurgical Adhesions1 PDFTito AlhoNo ratings yet
- Alo AjogDocument1 pageAlo AjogelenNo ratings yet
- b2 20Document6 pagesb2 20elenNo ratings yet
- Pituitary Tumors BrochureDocument20 pagesPituitary Tumors BrochureAnonymous M6HzvK6bNo ratings yet
- Amenorrhoea Long Version PDFDocument7 pagesAmenorrhoea Long Version PDFelenNo ratings yet
- Network Termination Unit STU4: Suppor Ting SHDSL - BisDocument2 pagesNetwork Termination Unit STU4: Suppor Ting SHDSL - BisНатальяNo ratings yet
- BA (Hons) Philosophy CurriculumDocument123 pagesBA (Hons) Philosophy CurriculumDARSHAN RAAJANNo ratings yet
- TG SkripsiDocument138 pagesTG SkripsiYudanto SetyoNo ratings yet
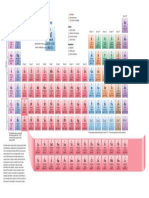
- Periodic TableDocument1 pagePeriodic TableChemist MookaNo ratings yet
- Testing The AdapterDocument8 pagesTesting The AdapterrejnanNo ratings yet
- Valuation and Risk ModelsDocument226 pagesValuation and Risk Models1690295017qq.comNo ratings yet
- CH3 SolutionsDocument40 pagesCH3 SolutionsRonelNo ratings yet
- Discoverer Installation and Integration With EBSDocument25 pagesDiscoverer Installation and Integration With EBSRajendra PrasadNo ratings yet
- Body Fat PercentageDocument7 pagesBody Fat Percentagegurveer singhNo ratings yet
- PDCT - Hydraulic Torque Wrench - Hangzhou Penad Machinery Co.,LtdDocument4 pagesPDCT - Hydraulic Torque Wrench - Hangzhou Penad Machinery Co.,LtdQS BMDSNo ratings yet
- Typescript Cheat Sheet: by ViaDocument2 pagesTypescript Cheat Sheet: by ViapbecicNo ratings yet
- Effects of Osteoarthritis and Fatigue On Proprioception of The Knee JointDocument5 pagesEffects of Osteoarthritis and Fatigue On Proprioception of The Knee JointRosaneLacerdaNo ratings yet
- Basic use of datum planes in Creo ParametricDocument8 pagesBasic use of datum planes in Creo ParametricKartik BhararaNo ratings yet
- Smart AntennasDocument40 pagesSmart AntennasMeeraNo ratings yet
- Quantitative Method Problem SetDocument10 pagesQuantitative Method Problem SetConstanceNo ratings yet
- MBA (Travel & Tourism) 1st Year Sylabus 2020-21 - 28th SeptDocument34 pagesMBA (Travel & Tourism) 1st Year Sylabus 2020-21 - 28th SeptHimanshuNo ratings yet
- Ldp-105m150 Moso Test ReportDocument17 pagesLdp-105m150 Moso Test ReportzecyberNo ratings yet
- Doubble EncriptionDocument60 pagesDoubble Encriptiondeepak kumarNo ratings yet
- Model For Calculating The Refractive Index of DiffDocument5 pagesModel For Calculating The Refractive Index of DiffNANNo ratings yet
- Dynamic Programming Algorithm Explained in ECE 551 LectureDocument11 pagesDynamic Programming Algorithm Explained in ECE 551 Lectureadambose1990No ratings yet
- Microelectronic Circuit Design 5th Edition Jaeger Blalock Solution ManualDocument21 pagesMicroelectronic Circuit Design 5th Edition Jaeger Blalock Solution Manualruth100% (23)
- House of CardsDocument2 pagesHouse of CardsHello misterNo ratings yet
- CH1 The Foundations - Logic and ProofsDocument106 pagesCH1 The Foundations - Logic and ProofsMOHAMED BACHARNo ratings yet
- COSC 2307: Sub-QueriesDocument23 pagesCOSC 2307: Sub-QueriesBhavikDaveNo ratings yet
- P&ID ManualDocument35 pagesP&ID Manualdharan kumarNo ratings yet
- ScanKromsator ManualDocument9 pagesScanKromsator ManualcensoredchapterNo ratings yet