Professional Documents
Culture Documents
zdcS253 PDF
Uploaded by
Ah.FaruqOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
zdcS253 PDF
Uploaded by
Ah.FaruqCopyright:
Available Formats
D I A B E T E S P R O G R E S S I O N , P R E V E N T I O N , A N D T R E A T M E N T
Insulin Therapy for Type 2 Diabetes
SANNE G. SWINNEN, MD tensification of insulin therapy in patients
JOOST B. HOEKSTRA, PHD with type 2 diabetes. Our aim is to assist
J. HANS DEVRIES, PHD clinicians in designing individualized
management plans for insulin therapy in
type 2 diabetic patients.
A
number of landmark randomized ation (ADA) recommendation of an A1C
clinical trials established that insu- target 7.0% seems the most balanced HUMAN INSULIN AND ITS
lin therapy reduces microvascular compromise at present (7). ANALOGS Insulin therapy with
complications (1,2). In addition, recent Another important conclusion of the the conventional mealtime and basal in-
follow-up data from the U.K. Prospective UKPDS was that the risk reductions in sulin preparations has many shortcom-
Diabetes Study (UKPDS) suggest that long-term complications were related to ings. First, the absorption of regular
early insulin treatment also lowers mac- the levels of glycemic control achieved, human insulin from the subcutaneous tis-
rovascular risk in type 2 diabetes (3). rather than to a specific glucose-lowering sue is slow, and the metabolic action takes
Whereas there is consensus on the need agent (1). This has left health care provid- effect only 30 60 min after injection and
for insulin, controversy exists on how to ers and patients with the difficult task of peaks after 23 h. Consequently, treat-
initiate and intensify insulin therapy. The choosing from the wide variety of glu- ment with regular insulin is associated
options for the practical implementation cose-lowering interventions currently with postmeal hyperglycemia and an in-
of insulin therapy are many. In this pre- available. When considering the effective- creased risk of late-postprandial hypogly-
sentation, we will give an overview of the ness, tolerability, and cost of the various cemia. Second, the conventional basal
evidence on the various insulin regimens diabetes treatments, insulin is not only NPH insulin has a distinct peak glucose-
commonly used to treat type 2 diabetes. the most potent, but also the most cost- lowering effect, has a duration of action
Secondary analyses of the aforemen- effective intervention (8). Although insu- considerably shorter than 24 h, and is ab-
tioned landmark trials endeavored to es- lin has no upper dose limit and numerous sorbed from the subcutaneous tissue at
tablish a glycemic threshold value below trials established that glycemic goals variable rates. These pharmacodynamic
which no complications would occur. could be attained by using adequate insu- limitations predispose users to elevated
The UKPDS found no evidence for such a lin doses (5,8), in clinical practice, many glucose levels before breakfast and noc-
threshold for A1C, but instead showed patients have elevated A1C levels and ex- turnal hypoglycemia (11,12). To over-
that better glycemic control was associ- perience years of uncontrolled hypergly- come these difficulties, insulin analogs
ated with reduced risks of complications cemia (9). Moreover, the Steno-2 Study with a modified amino acid sequence
over the whole glycemic range (the lower demonstrated that only a minority of pa- from the human insulin molecule were
the better) (4). For the management of tients reached the intensive A1C target of developed. The three rapid-acting ana-
type 2 diabetes, this resulted in the rec- 6.5%, compared with a far greater per- logs (aspart, glulisine, lispro) are ab-
ommendation to maintain glycemic lev- centage of patients who reached the re- sorbed more quickly than regular insulin
els as close to the nondiabetic range as spective intensive treatment goals for because of reduced self-association. Their
possible (5). However, in contrast to the blood pressure and serum lipid levels onset of action is within 15 min after sub-
UKPDS, the Kumamoto study observed a (10). Apparently, the initiation and inten- cutaneous injection, and they have a
threshold, with no exacerbation of micro- sification of insulin therapy is not as faster and greater peak action. Insulin
vascular complications in patients with straightforward and simple as we had glargine, the first long-acting insulin ana-
type 2 diabetes whose A1C was 6.5%, hoped. In accordance with the ADA and log to reach the market, was initially pro-
suggesting no additional benefit in lower- the European Association for the Study of claimed to have the ideal peakless,
ing A1C below this level (2). Moreover, Diabetes (EASD) (5,7), we advocate an al- nearly 24-h duration of action (13). How-
the intensive glycemia treatment arm of gorithmic approach for the start and ad- ever, these initial pharmacodynamic
the Action to Control Cardiovascular Risk justment of insulin treatment, with studies raised some criticism, and it
in Diabetes (ACCORD) study, targeting modifications for individual patients as should be concluded that there is no such
A1C 6.0%, was discontinued because needed. This review contains an overview thing as a peakless insulin preparation
of higher mortality in this group com- of the currently available insulin prepara- (12,14,15). Nevertheless, both long-
pared with the standard therapy group tions and an outline of the merits and dis- acting insulin analogs (detemir and
targeting A1C from 7.0 to 7.9% (6). advantages of the various regimens glargine) have a limited peak effect and a
Therefore, the American Diabetes Associ- commonly used for the initiation and in- longer mean duration of action compared
with NPH insulin (with glargine having a
From the Department of Internal Medicine, Academic Medical Center, Amsterdam, the Netherlands.
slightly longer action than detemir
Corresponding author: Sanne G. Swinnen, s.g.swinnen@amc.uva.nl. [13,16,17]).
The publication of this supplement was made possible in part by unrestricted educational grants from Eli It was expected that the rapid-acting
Lilly, Ethicon Endo-Surgery, Generex Biotechnology, Hoffmann-La Roche, Johnson & Johnson, LifeScan, and long-acting analogs, which more
Medtronic, MSD, Novo Nordisk, Pfizer, sanofi-aventis, and WorldWIDE. closely approximate physiological insulin
DOI: 10.2337/dc09-S318
2009 by the American Diabetes Association. Readers may use this article as long as the work is properly secretion, would confer important clini-
cited, the use is educational and not for profit, and the work is not altered. See http://creativecommons. cal benefits (11). With respect to type 2
org/licenses/by-nc-nd/3.0/ for details. diabetes, the topic of this review, it is im-
care.diabetesjournals.org DIABETES CARE, VOLUME 32, SUPPLEMENT 2, NOVEMBER 2009 S253
Insulin therapy for type 2 diabetes
portant to note that most patients with insulin groups than in the intensive oral price of a 10-ml vial of the long-acting
type 2 diabetes have residual endogenous therapy group. However, Wengs findings insulin analogs is $105 compared with
insulin secretion in the context of insulin need to be confirmed, and also for reasons $53 for a vial of NPH insulin (31). In this
resistance. Therefore, the rationale for im- of practicality and patients acceptance, respect, clinicians should realize that
itating the insulin secretion pattern of hu- we advocate stepwise diabetes treatment, when they stop prescribing conventional
man physiology is less convincing than in provided that an A1C of 7.0% serves as insulin preparations, with established
type 1 diabetes. Indeed, in patients with a call to action to initiate or change ther- beneficial effects, they provide a pretext
type 2 diabetes, the rapid-acting analogs apy (5). Moreover, the response to this for the manufacturers to withdraw these
were not found to be superior to regular call should be swift; given the great (cost-) drugs from the market. Recent examples
insulin in reducing A1C levels or rates of effectiveness, we advocate the initiation of of such industry responses to low demand
overall hypoglycemia (18). The clinical insulin when glycemic goals are not at- are the withdrawal of Novolin R penfills
benefits of the long-acting insulin analogs tained after 23 months of maximally in the U.K. and of Novolin 70/30 in sev-
compared with NPH insulin are limited to dosed dual oral therapy. For patients in- eral European countries. Thus, to recapit-
a reduction in (nocturnal) hypoglycemia tolerant to one or more oral glucose- ulate, given its cost-effectiveness, we
(19). lowering agents and who do not achieve consider NPH insulin the preferred agent
glycemic control with oral monotherapy, for the initiation of insulin therapy in type
WHEN SHOULD INSULIN as well as those with a personal prefer- 2 diabetes. However, if dose titration is
THERAPY BE INITIATED? Type ence, earlier initiation of insulin is indi- limited by (nocturnal) hypoglycemia, a
2 diabetes is a progressive disease, and cated. It is noteworthy that rapid addition switch to a long-acting insulin analog
thus, ultimately this question will arise for of insulin therapy is supported by numer- should be tried.
many of our patients. Unfortunately, ous studies showing improved treatment There is doubt as to whether a once-
there is no unequivocal answer, which satisfaction and quality-of-life for type 2 daily dose of insulin detemir will help as
was nicely illustrated by a recent interac- diabetic patients who had started using many people achieve good control as
tive case vignette. The polling results insulin (25,26). NPH insulin and glargine. In a treat-to-
demonstrated once again that the man- target trial with twice-daily detemir ad-
agement of patients with type 2 diabetes HOW SHOULD INSULIN ministration, an end point A1C of 6.8%
uncontrolled by two oral glucose- THERAPY BE INITIATED? was reached (28). In other studies, a sec-
lowering agents is controversial. Further- ond daily detemir injection was required
more, the preferred treatment option was Basal insulin in 34 55% of study subjects because of
found to be related to the respondents The treat-to-target clinical trials estab- predinner hyperglycemia or nocturnal
locations and self-reported specialties lished that the addition of basal insulin to hypoglycemia (29,32). In the only re-
(20). existing oral glucose-lowering therapy ported trial that investigated the efficacy
Traditionally, there has been a step- achieves good glycemic control in the ma- of once-daily insulin detemir, A1C re-
wise introduction of glucose-lowering in- jority of patients with type 2 diabetes mained above the currently recom-
terventions, with the final step of insulin (2729). According to the ADA/EASD al- mended glycemic goal with an end point
therapy being administered 10 15 years gorithm for the management of type 2 di- level of 7.4%, both for NPH insulin and
after diagnosis (8). Both patients and phy- abetes, insulin could be initiated with detemir (33), compared with an end of
sicians are often reluctant to start insulin either once-daily NPH insulin or a long- study A1C 7.0% with once-daily
because of fears of painful injections, hy- acting insulin analog (5). For several rea- glargine and NPH in the original Treat-to-
poglycemia, and weight gain (21,22). Ad- sons, we consider NPH insulin the Target Trial (27). Rather than possible in-
ditional reasons for psychological insulin preferred option. As previously men- sufficiency of a once-daily dose of insulin
resistance among patients are negative tioned, the relative benefit of the long- detemir, these discrepant outcomes are
beliefs about insulin treatment perma- acting insulin analogs is limited to a likely to be explained by diversity in study
nence, restrictiveness, low self-efficacy, reduction in (nocturnal) hypoglycemia design, such as different titration targets
personal failure, and illness severity (22). (19). Moreover, this advantage is relevant and titration frequency. This is supported
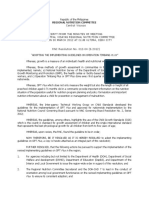
Drawback of the stepwise approach is that to only a minority, since most patients by Figs. 1A and B, which show the rela-
the introduction of successive interven- with type 2 diabetes starting insulin ther- tionship between the reduction in A1C
tions after treatment failure is often de- apy do not experience hypoglycemia at all level and end point insulin dose, and be-
layed, exposing patients to many years of (12). A recent meta-analysis that included tween A1C reduction and the frequency
uncontrolled hyperglycemia (9). Another six randomized comparisons of NPH and of patient contact, respectively, in nine
reason for a more rapid response to treat- glargine found event rates for self- randomized trials investigating insulin
ment failure is that lowering glycemia has monitoring of blood glucose (SMBG) con- initiation with basal insulin (2729,32
been shown to improve insulin resistance firmed symptomatic hypoglycemia 65 37). Both graphs show clear dose-
as well as endogenous insulin secretion mg/dl of only 138 and 91 events per 100 response relationships, suggesting that
(23). This was recently confirmed by patient-years for these insulins, respec- substantial decreases in A1C can be
Weng et al. (24) who found that a brief tively, in insulin-naive type 2 diabetic pa- achieved, provided that the daily insulin
course of insulin therapy in subjects with tients who achieved an A1C of 7.0% (30). dose and the contact frequency are ade-
newly diagnosed type 2 diabetes not only Finally, in this era of relentlessly increas- quate. The only way to finally determine
restored, but also maintained, -cell ing incidence rates for type 2 diabetes, whether once-daily detemir injection is
function, resulting in prolonged glycemic physicians cannot afford to disregard the appropriate for the treatment of type 2
remission. Interestingly, remission rates elevated cost of the newer insulin prepa- diabetes is to conduct a clinical trial, ide-
were significantly higher in the intensive rations. In the U.S., the average retail ally comparing once-daily detemir and
S254 DIABETES CARE, VOLUME 32, SUPPLEMENT 2, NOVEMBER 2009 care.diabetesjournals.org
Swinnen, Hoekstra, and DeVries
Figure 1Relationships between mean end point daily insulin dose
(A) and the frequency of patient contact (clinical visits and telephone
contacts combined) (B) and mean reduction in A1C, and between mean
end point daily insulin dose and mean weight gain (C), during nine
randomized trials investigating insulin initiation with NPH insulin,
insulin detemir, or insulin glargine. Included studies are Bretzel et al.
(34), Fritsche et al. (35), Hermansen et al. (28), Holman et al. (32),
Philis-Tsimikas et al. (33), Riddle et al. (27), Rosenstock et al. (29),
Yki-Jarvinen et al. (36), and Yki-Jarvinen et al. (37) (A and C). B does
not include Holman, since this publication did not specify the number of
interim telephone contacts. Two trials (28,35) did not report mean end
point daily insulin dose as units per kilogram per day. We calculated the
desired figures from the mean end point dose reported as units per day
and mean body weight at study end. Three studies (Riddle and the two
studies of Yki-Jarvinen [27,36,37]) did not report reduction in A1C. We
calculated these values from mean baseline and end point A1C levels.
glargine in patients with baseline A1C lev- solely included patients at high risk for car- insulin glargine found greater reductions in
els of 8.5%. Such a study could also diovascular disease, in whom low A1C lev- A1C and nocturnal hypoglycemia with
assess whether higher detemir dosages are els were reached by using up to four or five morning compared with evening injection
needed to obtain the same level of glyce- different classes of glucose-lowering drugs. (35), whereas a larger comparison of morn-
mic control as with insulin glargine, as In contrast, in less selected patients treated ing versus evening glargine with an identi-
was demonstrated in two of the aforemen- with stable doses of one or two oral agents, cal study design did not find any difference
tioned studies in which detemir was ad- simple titration algorithms targeting fasting (both studies investigated this issue against
ministered twice daily (28,29,38). This plasma glucose 100 mg/dl (5.6 mmol/l) a background of glimepiride once daily)
trial could also confirm the proclaimed can safely achieve A1C of 7.0% (27). A pa- (41). A morning administration of insulin
reduction in weight gain associated with tient-driven algorithm, with patients in- detemir was associated with lower glucose
insulin detemir. creasing their insulin dose by 2 or 3 units levels during the day and a trend toward a
every 3 days, as long as their fasting plasma reduced risk of nocturnal hypoglycemia
Titration and timing of basal insulin glucose remains above target, constitutes a compared with evening injection (33).
After the recent unexpected finding of in- practical approach that has been shown to From these discrepant data, it can be con-
creased mortality in the intensive glucose- be equally or more effective than physician- cluded that when nocturnal hypoglycemia
lowering therapy group of the ACCORD led titration (39,40). limits dose titration of evening detemir or
study, which might be partly related to the Regarding the timing of injection in glargine, administration in the morning
rate of the reduction in A1C (6), clinicians once-daily basal insulin regimens, adminis- could be attempted.
may now be more reserved to lower glucose tration of NPH in the evening appears to be
levels promptly. However, we still feel that superior to morning injection (11,25). Other options for the initiation of
in addition to timely initiation, rapid titra- Studies examining the injection time of the insulin therapy
tion of the dose is indispensable for success- long-acting insulin analogs showed con- The recent Treating to Target in type 2
ful insulin therapy. The ACCORD study flicting results. One study conducted with Diabetes (4-T) study compared the intro-
care.diabetesjournals.org DIABETES CARE, VOLUME 32, SUPPLEMENT 2, NOVEMBER 2009 S255
Insulin therapy for type 2 diabetes
duction of basal insulin at bedtime to in- (CODHy) meeting, the rationale for com- How should insulin therapy be
sulin initiation with either biphasic bining insulin with oral therapy is mini- intensified?
insulin twice daily or prandial insulin be- mization of the adverse effects of insulin The available options for additional insu-
fore meals (32). The biphasic and pran- treatment, i.e., hypoglycemia and weight lin injections include a second injection of
dial insulin regimens provided better gain (44). Combination of insulin with basal insulin, prandial insulin before one
glycemic control than once-daily basal in- metformin is indeed associated with bet- or more meals, or a switch to biphasic
sulin (escalated to twice daily in 34% of ter glycemic control, fewer hypoglycemic insulin. The choice between intensifica-
patients) but at the expense of increased events, and less weight gain than treat- tion of basal insulin versus the introduc-
risks of hypoglycemia and weight gain. ment with insulin alone (45). Therefore, tion of prandial or biphasic insulin should
Although biphasic insulin reduced A1C metformin should be continued when pa- be individualized based on patients diur-
levels to the same extent as prandial insu- tients are initiated on insulin therapy (i.e., nal blood glucose profiles. When consid-
lin, the latter regimen was associated with providing there are no intolerable side ef- ering the profiles obtained with NPH
the most hypoglycemic episodes and the fects). Data concerning the combination insulin or long-acting insulin analog once
highest weight gain (32). Therefore, and daily, the effect appears to wane during
of insulin with either sulfonylureas alone,
considering that to date there is no clinical the day, even in patients starting insulin
or with both metformin and sulfonyl-
trial evidence supporting the specific low- therapy, i.e., with remaining endogenous
ureas, compared with insulin-alone treat-
ering of postprandial glucose levels when insulin secretion (33,37,48). These pa-
aiming to lower cardiovascular risk in ment regimens, are ambiguous (46). The tients could benefit from adding a second
type 2 diabetes, initiation with prandial only consistent advantage of such com- injection of basal insulin (48). However,
insulin is generally not a first-choice ap- bined therapy is reduced insulin dose re- in the context of declining endogenous
proach when starting insulin in type 2 di- quirements, which may result in less daily insulin secretion, daytime hyperglycemia
abetic patients. This was confirmed by a injections, easier dose titration, and im- is usually related to elevated postprandial
recently reported direct comparison of proved compliance (46). However, these glucose levels, favoring the initiation of
once-daily insulin glargine versus thrice- potential benefits must be balanced prandial or biphasic insulin.
daily insulin lispro in insulin-naive pa- against the side effects and higher cost of Two recent studies established that in
tients (34). Finally, also regarding continuing sulfonylureas together with patients not achieving adequate glycemic
feasibility in clinical practice and patients metformin compared with treatment with control with once-daily basal insulin, bas-
acceptance, three injections per day is the metformin and NPH insulin alone al-bolus therapy results in greater A1C re-
least attractive option for initiation of in- although not versus long-acting insulin ductions than biphasic insulin twice or
sulin therapy. analogs and metformin alone (31,46) thrice daily (49,50). However, when a
Although many are accustomed to and the possibility of reduced patient ad- more gradual intensification of insulin
initiation with biphasic insulin, we gener- herence when increasing numbers of pills treatment is preferred, patients can be
ally recommend the addition of once- are prescribed (47). An ongoing random- switched to biphasic insulin two, and
daily basal insulin to oral therapy for ized trial comparing the continuation of subsequently three, times daily. The latter
several reasons. First, the lower A1C lev- sulfonylureas in combination with met- regimen has been shown to significantly
els reached with biphasic insulin comes at formin and insulin glargine versus dis- improve A1C levels of patients previously
the expense of increased risks of hypogly- continuation of sulfonylureas with this treated with insulin glargine (50).
cemia and weight gain (32,42,43). Sec- combination regimen in insulin-naive Whether stepwise introduction of meal-
ond, and as aforementioned, trials with type 2 diabetic patients will hopefully time injections is as safe and effective as
systematic dose titration demonstrated provide further evidence regarding this is- the rapid initiation of a full basal-bolus
that once-daily basal insulin achieves the sue (ISRCTN29335793: www.controlled- regimen is currently under investigation
currently recommended glycemic levels trials.com). (51).
in many patients with type 2 diabetes Finally, regarding the choice of pran-
(27,29). In this respect, it has frequently dial insulin, rapid-acting insulin analogs
been argued that in patients with badly are not superior to regular insulin in re-
INTENSIFICATION OF
controlled hyperglycemia (e.g., A1C ducing A1C levels or rates for overall and
INSULIN THERAPY
8.5% at the start of insulin therapy), nocturnal hypoglycemia, despite improv-
treatment with once-daily basal insulin ing postprandial control (18). In some
When should insulin therapy be
alone would not attain glycemic goals studies, treatment with rapid-acting ana-
(11,32,33). However, the LANMET study intensified? logs was associated with fewer severe hy-
proved otherwise. In this clinical trial, Because of progressive -cell decline, poglycemic episodes and improved
A1C levels decreased from 9.1% at base- treatment with once-daily basal insulin treatment satisfaction (18), the latter
line to 7.1% with combination therapy of alone will eventually fail to maintain gly- probably being related to increased con-
bedtime insulin glargine or NPH insulin cemic control in a substantial number of venience because of injection immedi-
and metformin (36). Finally, it seems patients with type 2 diabetes. When the ately before meals. In conclusion, there is
likely that insulin initiation by means of recommended A1C level of 7.0% is not no compelling reason to overall favor rap-
one (basal) injection may also facilitate reached, or maintained despite successful id-acting insulin analogs over regular in-
patients acceptance of insulin initiation. basal insulin dose titration maintaining sulin in type 2 diabetes. Whereas in some
fasting plasma glucose 100 mg/dl, or countries the price of rapid-acting analogs
Combined therapy with oral agents when aggressive titration is limited by hy- has been lowered to the level of regular
As discussed at the first Controversies in poglycemia, treatment should be intensi- insulin, in others, it remains around twice
Obesity, Diabetes and Hypertension fied by adding insulin injections. as high (31).
S256 DIABETES CARE, VOLUME 32, SUPPLEMENT 2, NOVEMBER 2009 care.diabetesjournals.org
Swinnen, Hoekstra, and DeVries
Continuous subcutaneous insulin apy, attempts to attain A1C goals should iological insulin secretion pattern is less
infusion not be hampered too much by concerns convincing than in type 1 diabetes.
In patients with type 2 diabetes already about hypoglycemia. However, iatrogenic Glycemic treatment should be step-
using at least one daily insulin injection, hypoglycemia appears to become a more wise with swift introduction of successive
the introduction of intensive insulin ther- frequent problem at the insulin-deficient interventions after treatment failure (i.e.,
apy with continuous subcutaneous insu- stage of the disease, warranting more vig- A1C 7.0%). Insulin should be initiated
lin infusion resulted in comparable ilance as the disease advances (54). when A1C is 7.0% after 23 months of
glycemic control, weight gain, and hypo- dual oral therapy. The preferred regimen
glycemia risk as multiple daily injection Weight gain for insulin initiation in type 2 diabetes is
therapy (52,53). Although continuous The 2- to 4-kg increase in body weight once-daily basal insulin. In addition to
subcutaneous insulin infusion was asso- associated with insulin therapy has tradi- timely initiation, rapid titration of the
ciated with greater improvements in treat- tionally been explained by reductions of dose is indispensable for successful insu-
ment satisfaction in one study (53), we glucosuria and resting energy expendi- lin therapy. Hypoglycemia risk is very low
recommend that its use be restricted to ture when glycemic control is improved among type 2 diabetic patients just start-
selected patients in experienced centers (5,46). Other explanations are snacking ing insulin therapy, making NPH insulin
only. to prevent, or in response to, hypoglyce- the most cost-effective drug.
mia or restoration of the weight loss usu- When glycemic goals are not attained
DRAWBACKS OF INSULIN ally preceding insulin initiation to the despite successful basal insulin dose titra-
THERAPY weight before onset of diabetes. In con- tion (i.e., fasting plasma glucose 100
trast, a recent study found that the mean mg/dl), or when titration is limited by hy-
Hypoglycemia weight gain of 1.8 kg in 23 type 2 diabetic poglycemia, treatment should be intensi-
Intensive glucose-lowering therapy inev- patients during the first 6 months of insu- fied by addition of prandial or biphasic
itably results in an increased rate of lin therapy was not accompanied by a insulin.
hypoglycemia, which was once again con- change in glucosuria, resting energy ex-
firmed in the recent ACCORD study with penditure, or physical activity. The au-
annualized rates of hypoglycemic epi- thors concluded that increased energy Acknowledgments S.G.S. is employed by
the Department of Internal Medicine of the
sodes requiring medical assistance of 3.1 intake was the only plausible explanation
Academic Medical Center, partly through
and 1.0% in the intensive and standard for the observed weight increments (62). funding from Novo Nordisk and sanofi-
therapy groups, respectively (6). Iatro- Although the mechanisms underlying in- aventis for the conduct of clinical trials. J.B.H.
genic hypoglycemia hampers tight glyce- sulin-associated weight gain are still not has received honoraria for consultancy work
mic control and is considered the limiting fully understood, it is thought to be pro- from Novartis and sanofi-aventis. J.H.D. has
factor in diabetes management (54). portional to the number of insulin injec- received honoraria for consultancy work as
Opinions are divided on the extent of tions, or the total daily insulin dose well as research funding from Novo Nordisk
the problem, with cited event rates for se- (32,45,46). Interestingly, when consider- and sanofi-aventis.
vere hypoglycemia in insulin-treated type ing studies investigating basal insulin ini- No other potential conflicts of interest rele-
2 diabetic patients ranging from between tiation in type 2 diabetes, we found no vant to this article were reported.
1 and 3 (5) to between 10 and 73 per 100 evidence for such a dose-response rela-
patient-years (55). Of note, the relatively tionship (Fig. 1C). References
low rates were found in clinical trials Finally, when directly comparing the 1. U.K. Prospective Diabetes Study (UKPDS)
(2,56), whereas the higher figures were mean increases in body weight during in- Group. Intensive blood-glucose control
reported in retrospective and population- sulin initiation with NPH insulin versus with sulphonylureas or insulin compared
based studies (5759). The difference is long-acting insulin analogs, insulin with conventional treatment and risk of
probably explained by varying durations glargine is associated with similar weight complications in patients with type 2 di-
of disease or insulin therapy in the cited gain (27,3537). Treatment with insulin abetes (UKPDS 33). Lancet 1998;352:
studies. The risks of mild and severe hy- detemir, on the other hand, appears to 837 853
poglycemia are low among type 2 diabetic result in less weight gain than NPH insu- 2. Ohkubo Y, Kishikawa H, Araki E, Miyata T,
Isami S, Motoyoshi S, Kojima Y, Furuyoshi
patients just beginning insulin therapy lin (28,33). However, considering the N, Shichiri M. Intensive insulin therapy pre-
(30) and appear to increase with increas- limited magnitude of the reported weight- vents the progression of diabetic microvas-
ing durations of diabetes and insulin sparing effect, we still recommend NPH cular complications in Japanese patients
treatment (5759). insulin for the initiation of insulin therapy with non-insulin-dependent diabetes melli-
To conclude, in type 2 diabetes, the in patients with type 2 diabetes. tus: a randomized prospective 6-year study.
frequency of hypoglycemia is generally Diabetes Res Clin Pract 1995;28:103117
lower than that in type 1 diabetes (54). CONCLUSIONS Although insu- 3. Holman RR, Paul SK, Bethel MA, Mat-
This is presumably the result of relative lin has no upper dose limit and numer- thews DR, Neil HA. 10-year follow-up of
protection of type 2 diabetic patients ous trials established that glycemic intensive glucose control in type 2 diabe-
against hypoglycemia by residual endog- goals can be attained by using adequate tes. N Engl J Med 2008;359:15771589
4. Stratton IM, Adler AI, Neil HA, Matthews
enous (i.e., physiologically regulated) in- doses, in clinical practice, many pa- DR, Manley SE, Cull CA, Hadden D,
sulin and glucagon secretion, insulin tients experience years of uncontrolled Turner RC, Holman RR. Association of
resistance, and higher glycemic thresh- hyperglycemia. glycaemia with macrovascular and micro-
olds for counterregulatory and symptom- Because most type 2 diabetic patients vascular complications of type 2 diabetes
atic responses to hypoglycemia (60,61). have residual endogenous insulin secre- (UKPDS 35): prospective observational
Therefore, when initiating insulin ther- tion, the rationale for imitating the phys- study. BMJ 2000;321:405 412
care.diabetesjournals.org DIABETES CARE, VOLUME 32, SUPPLEMENT 2, NOVEMBER 2009 S257
Insulin therapy for type 2 diabetes
5. Nathan DM, Buse JB, Davidson MB, detemir at steady state in type 1 diabetes: parallel, treat-to-target trial comparing in-
Ferrannini E, Holman RR, Sherwin R, a double-blind, randomized, crossover sulin detemir with NPH insulin as add-on
Zinman B. Medical management of study. Diabetes Care 2007;30:2447-2452 therapy to oral glucose-lowering drugs in
hyperglycemia in type 2 diabetes: a con- 18. Siebenhofer A, Plank J, Berghold A, Jeitler insulin-naive people with type 2 diabetes.
sensus algorithm for the initiation and K, Horvath K, Narath M, Gfrerer R, Pieber Diabetes Care 2006;29:1269 1274
adjustment of therapy: a consensus TR. Short acting insulin analogues versus 29. Rosenstock J, Davies M, Home P, Larsen J,
statement of the American Diabetes As- regular human insulin in patients with di- Koenen C, Schernthaner G. A random-
sociation and the European Association abetes mellitus. Cochrane Database Syst ised, 52-week, treat-to-target trial com-
for the Study of Diabetes. Diabetes Care Rev 2006:CD003287 paring insulin detemir with insulin
2009;32:193203 19. Horvath K, Jeitler K, Berghold A, Ebrahim glargine when administered as add-on to
6. Action to Control Cardiovascular Risk in SH, Gratzer TW, Plank J, Kaiser T, Pieber glucose-lowering drugs in insulin-naive
Diabetes Study Group. Effects of intensive TR, Siebenhofer A. Long-acting insulin people with type 2 diabetes. Diabetologia
glucose lowering in type 2 diabetes. analogues versus NPH insulin (human 2008;51:408 416
N Engl J Med 2008;358:25452559 isophane insulin) for type 2 diabetes mel- 30. Mullins P, Sharplin P, Yki-Jarvinen H,
7. American Diabetes Association: Stan- litus. Cochrane Database Syst Rev 2007: Riddle MC, Haring HU. Negative bino-
dards of medical care in diabetes: 2009. CD005613 mial meta-regression analysis of com-
Diabetes Care 2009;32:S13S61 20. Halperin F, Ingelfinger JR, McMahon GT. bined glycosylated hemoglobin and
8. Nathan DM. Initial management of glyce- Management of type 2 diabetes: polling hypoglycemia outcomes across eleven
mia in type 2 diabetes mellitus. N Engl results. N Engl J Med 2008;358:e8 phase III and IV studies of insulin glargine
J Med 2002;347:13421349 21. Nakar S, Yitzhaki G, Rosenberg R, Vinker compared with Neutral Protamine Hage-
9. Brown JB, Nichols GA, Perry A. The bur- S. Transition to insulin in type 2 diabetes: dorn insulin in type 1 and type 2 diabetes
den of treatment failure in type 2 diabetes. family physicians misconception of pa- mellitus. Clin Ther 2007;29:16071619
Diabetes Care 2004;27:15351540 tients fears contributes to existing barri- 31. Drug Prices. Available from http://www.
10. Gaede P, Vedel P, Larsen N, Jensen GVH, ers. J Diabetes Complications 2007; drugstore.com. Accessed 17 November
Parving HH, Pedersen O. Multifactorial 21:220 226 2008
intervention and cardiovascular disease in 22. Polonsky WH, Fisher L, Guzman S, Villa- 32. Holman RR, Thorne KI, Farmer AJ, Da-
patients with type 2 diabetes. N Engl Caballero L, Edelman SV. Psychological vies MJ, Keenan JF, Paul S, Levy JC,
J Med 2003;348:383393 insulin resistance in patients with type 2 Group TS. Addition of biphasic, prandial,
11. Hirsch IB. Insulin analogues. N Engl diabetes: the scope of the problem. Dia- or basal insulin to oral therapy in type 2
J Med 2005;352:174 183 betes Care 2005;28:25432545 diabetes. N Engl J Med 2007;357:1716
12. Holleman F, Gale E. Nice insulins, pity 23. Yki-Jarvinen H, Esko N, Eero H, Marja- 1730
about the evidence. Diabetologia 2007; Riitta T. Clinical benefits and mechanisms 33. Philis-Tsimikas A, Charpentier G, Clau-
50:17831790 of a sustained response to intermittent in- son P, Ravn GM, Roberts VL, Thorsteins-
13. Lepore M, Pampanelli S, Fanelli C, Por- sulin therapy in type 2 diabetic patients son B. Comparison of once-daily insulin
cellati F, Bartocci L, Di Vincenzo A, Cor- with secondary drug failure. Am J Med detemir with NPH insulin added to a reg-
doni C, Costa E, Brunetti P, Bolli GB. 1988;84:185192 imen of oral antidiabetic drugs in poorly
Pharmacokinetics and pharmacodynam- 24. Weng J, Li Y, Xu W, Shi L, Zhang Q, Zhu controlled type 2 diabetes. Clin Ther
ics of subcutaneous injection of long-act- D, Hu Y, Zhou Z, Yan X, Tian H, Ran X, 2006;28:1569 1581
ing human insulin analog glargine, NPH Luo Z, Xian J, Yan L, Li F, Zeng L, Chen Y, 34. Bretzel RG, Nuber U, Landgraf W, Owens
insulin, and ultralente human insulin and Yang L, Yan S, Liu J, Li M, Fu Z, Cheng H. DR, Bradley C, Linn T. Once-daily basal
continuous subcutaneous infusion of in- Effect of intensive insulin therapy on beta- insulin glargine versus thrice-daily pran-
sulin lispro. Diabetes 2000;49:2142- cell function and glycaemic control in dial insulin lispro in people with type 2
2148 patients with newly diagnosed type 2 diabetes on oral hypoglycaemic agents
14. DeVries JH. Pharmacokinetic and glu- diabetes: a multicentre randomised parallel- (APOLLO): an open randomised con-
codynamic variability: assessment of in- group trial. Lancet 2008;371:1753-1760 trolled trial. Lancet 2008;371:10731084
sulin glargine, NPH insulin and insulin 25. Yki-Jarvinen H, Kauppila M, Kujansuu E, 35. Fritsche A, Schweitzer MA, Haring HU.
ultralente in healthy volunteers using a Lahti J, Marjanen T, Niskanen L, Rajala S, Glimepiride combined with morning in-
euglycaemic clamp technique: response Ryysy L, Salo S, Seppala P. Comparison sulin glargine, bedtime neutral Protamine
to Scholtz HE et al. Diabetologia 2006;49: of insulin regimens in patients with Hagedorn insulin, or bedtime insulin
11251126 non-insulin-dependent diabetes mellitus. glargine in patients with type 2 diabetes.
15. Heise T, Pieber TR. Towards peakless, re- N Engl J Med 1992;327:1426 1433 Ann Intern Med 2003;138:952959
producible and long-acting insulins: an 26. Houlden R, Ross S, Harris S, Yale JF, 36. Yki-Jarvinen H, Kauppinen-Makelin R,
assessment of the basal analogues based Sauriol L, Gerstein HC. Treatment sat- Tiikkainen M, Vahatalo M, Virtamo H,
on isoglycaemic clamp studies. Diabetes isfaction and quality of life using an Nikkila K, Tulokas T, Hulme S, Hardy K,
Obes Metab 2007;9:648 659 early insulinization strategy with insulin McNulty S, Hanninen J, Levanen H, Lah-
16. Plank J, Bodenlenz M, Sinner F, Magnes glargine compared to an adjusted oral denpera S, Lehtonen R, Ryysy L. Insulin
C, Gorzer E, Regittnig W, Endahl LA, therapy in the management of type 2 dia- glargine or NPH combined with met-
Draeger E, Zdravkovic M, Pieber TR. betes: The Canadian INSIGHT study. Di- formin in type 2 diabetes: the LANMET
A double-blind, randomized, dose-re- abetes Res Clin Pract 2007;78:254 258 study. Diabetologia 2006;49:442 451
sponse study investigating the pharmaco- 27. Riddle MC, Rosenstock J, Gerich J. The 37. Yki-Jarvinen H, Dressler A, Ziemen M, for
dynamic and pharmacokinetic properties treat-to-target trial: randomized addition the HOE 901/3002 Study Group: Less
of the long-acting insulin analog detemir. of glargine or human NPH insulin to oral nocturnal hypoglycemia and better post-
Diabetes Care 2005;28:11071112 therapy of type 2 diabetic patients. Diabe- dinner glucose control with bedtime in-
17. Porcellati F, Rossetti P, Busciantella NR, tes Care 2003;26:3080 3086 sulin glargine compared with bedtime
Marzotti S, Lucidi P, Luzio S, Owens DR, 28. Hermansen K, Davies M, Derezinski T, NPH insulin during insulin combination
Bolli GB, Fanelli CG. Comparison of Martinez Ravn G, Clauson P, Home P, on therapy in type 2 diabetes. Diabetes Care
pharmacokinetics and dynamics of the behalf of the Levemir Treat-to-Target 2000;23:1130 1136
long-acting insulin analogs glargine and Study Group. A 26-week, randomized, 38. Swinnen SG, DeVries JH. Higher dose re-
S258 DIABETES CARE, VOLUME 32, SUPPLEMENT 2, NOVEMBER 2009 care.diabetesjournals.org
Swinnen, Hoekstra, and DeVries
quirements with insulin detemir in type 2 with insulin in type 2 diabetes. Diabetes factor in the glycaemic management of
diabetes: three cases and a review of the Care 2001;24:758 767 type I and type II diabetes. Diabetologia
literature. Diabetes Res Clin Pract 2009; 47. Massi-Benedetti M, Orsini-Federici M. 2002;45:937948
84:e24 e26 Treatment of type 2 diabetes with com- 55. Cryer PE. Management of hyperglycaemia
39. Davies M, Storms F, Shutler S, Bianchi- bined therapy: what are the pros and in type 2 diabetes: a consensus algorithm
Biscay M, Gomis R, for the AT.LANTUS cons? Diabetes Care 2008;31 (Suppl. 2): for the initiation and adjustment of ther-
Study Group. Improvement of glycemic S131S135 apy: response to Nathan DM et al. Diabe-
control in subjects with poorly controlled 48. DeVries JH, Nattrass M, Pieber TR. Refin- tes Care 2007;30:190 192
type 2 diabetes: comparison of two treat- ing basal insulin therapy: what have we 56. Abraira C, Colwell JA, Nuttall FQ, Sawin
ment algorithms using insulin glargine. learned in the age of analogues? Diabete CT, Nagel NJ, Comstock JP, Emanuele
Diabetes Care 2005;28:12821288 Metab Res Rev 2007;23:441 454 NV, Levin SR, Henderson W, Lee HS. Vet-
40. Selam JL, Koenen C, Weng W, Meneghini 49. Liebl A, Prager R, Binz K, Kaiser M, Ber- erans affairs cooperative study on glyce-
L. Improving glycemic control with insu- genstal R, Gallwitz B. Comparison of in- mic control and complications in type II
lin detemir using the 303 algorithm in in- sulin analogue regimens in people with diabetes (VA CSDM): results of the feasi-
sulin naive patients with type 2 diabetes: a type 2 diabetes mellitus in the PREFER bility trial. Diabetes Care 1995;18:1113
subgroup analysis of the US PREDICTIVE Study: a randomized controlled trial. Di- 1123
303 study. Curr Med Res Opin 2008;24: abetes Obes Metab 2009;11:4552 57. Donnelly LA, Morris AD, Frier BM, Ellis
1120 50. Rosenstock J, Ahmann AJ, Colon G, JD, Donnan PT, Durrant R, Band MM,
41. Standl E, Maxeiner S, Raptis S. Once-daily Scism-Bacon J, Jiang H, Martin S. Advanc- Reekie G, Leese GP. Frequency and pre-
insulin glargine administration in the ing insulin therapy in type 2 diabetes pre- dictors of hypoglycaemia in type 1 and
morning compared to bedtime in combi- viously treated with glargine plus oral insulin-treated type 2 diabetes: a popula-
nation with morning glimepiride in pa- agents: prandial premixed (insulin lispro tion-based study. Diabet Med 2005;22:
tients with type 2 diabetes: an assessment protamine suspension/lispro) versus bas- 749 755
of treatment flexibility. Horm Metab Res al/bolus (glargine/lispro) therapy. Diabe- 58. Henderson JN, Allen KV, Deary IJ, Frier
2006;38:172177 tes Care 2008;31:20 25 BM. Hypoglycaemia in insulin-treated
42. Malone JK, Kerr LF, Campaigne BN, Sa- 51. OSIRIS. Opposing step-by-step insulin re- type 2 diabetes: frequency, symptoms and
chson RA, Holcombe JH. Combined ther- inforcement to intensified strategy [article impaired awareness. Diabet Med 2003;
apy with insulin lispro mix 75/25 plus online], 2005. Available from http://www. 20:1016 1021
metformin or insulin glargine plus met- clinicaltrials.gov/ct2/show/NCT00174642? 59. MacLeod KM, Hepburn DA, Frier BM.
formin: a 16-week, randomized, open-la- termosiris&rank8. Accessed 17 No- Frequency and morbidity of severe hypo-
bel, crossover study in patients with type vember 2008 glycaemia in insulin-treated diabetic pa-
2 diabetes beginning insulin therapy. Clin 52. Herman WH, Ilag LL, Johnson SL, Martin tients. Diabet Med 1993;10:238 245
Ther 2004;26:2034 2044 CL, Sinding J, Al Harthi A, Plunkett CD, 60. Spyer G, Hattersley AT, MacDonald IA,
43. Raskin P, Allen E, Hollander P, Lewin A, LaPorte FB, Burke R, Brown MB, Halter Amiel S, MacLeod KM. Hypoglycaemic
Gabbay RA, Hu P, Bode B, Garber A, for JB, Raskin P. A clinical trial of continuous counter-regulation at normal blood glu-
the INITIATE Study Group. Initiating in- subcutaneous insulin infusion versus cose concentrations in patients with well
sulin therapy in type 2 diabetes: a com- multiple daily injections in older adults controlled type-2 diabetes. Lancet 2000;
parison of biphasic and basal insulin with type 2 diabetes. Diabetes Care 2005; 356:1970 1974
analogs. Diabetes Care 2005;28:260 265 28:1568 1573 61. Zammitt NN, Frier BM. Hypoglycemia in
44. Riddle MC. Combined therapy with insu- 53. Raskin P, Bode BW, Marks JB, Hirsch IB, type 2 diabetes: pathophysiology, fre-
lin plus oral agents: is there any advan- Weinstein RL, McGill JB, Peterson GE, quency, and effects of different treatment
tage? An argument in favor. Diabetes Care Mudaliar SR, Reinhardt RR. Continuous modalities. Diabetes Care 2005;28:
2008;31:S125S130 subcutaneous insulin infusion and multi- 2948 2961
45. Yki-Jarvinen H, Ryysy L. Comparison of ple daily injection therapy are equally ef- 62. Ryan M, Livingstone MB, Ducluzeau PH,
bedtime insulin regimens in patients with fective in type 2 diabetes: a randomized, Salle A, Genaitay M, Ritz P. Is a failure to
type 2 diabetes mellitus. Ann Intern Med parallel-group, 24-week study. Diabetes recognize an increase in food intake a key
1999;130:389 Care 2003;26:2598 2603 to understanding insulin-induced weight
46. Yki-Jarvinen H. Combination therapies 54. Cryer PE. Hypoglycaemia: the limiting gain? Diabetes Care 2008;31:448 450
care.diabetesjournals.org DIABETES CARE, VOLUME 32, SUPPLEMENT 2, NOVEMBER 2009 S259
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- GliclazideDocument5 pagesGliclazideGwyn RosalesNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Capitol University: College of Nursing Cagayan de Oro CityDocument2 pagesCapitol University: College of Nursing Cagayan de Oro CityChaine Agolito100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Unilab CSR PDFDocument24 pagesUnilab CSR PDFJennefer GemudianoNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Luborsky, Lester - Principles of Psychoanalytic Psychotherapy PDFDocument295 pagesLuborsky, Lester - Principles of Psychoanalytic Psychotherapy PDFMario Hernández Jr.No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Food Antioxidants - Nguyen Giang Yen ThoDocument3 pagesFood Antioxidants - Nguyen Giang Yen ThoYen Tho NguyenNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Dimensionity of EarthyDocument2 pagesDimensionity of EarthyErnest SUNDAYNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Gowrishankar Potturi: B.P.T, M.PT, M.I.A.P, M.I.A.C.PDocument24 pagesGowrishankar Potturi: B.P.T, M.PT, M.I.A.P, M.I.A.C.PMuhammad Luqmanulhakim Abu Bakar100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Programs and Events Run at National and Inter-National Level For Disaster MitigationDocument15 pagesPrograms and Events Run at National and Inter-National Level For Disaster MitigationRushiNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Grade 3 DLL Mapeh 3 q1 Week 3Document3 pagesGrade 3 DLL Mapeh 3 q1 Week 3Edza Formentera SasaritaNo ratings yet
- RNC Res. 012-04 s2012Document2 pagesRNC Res. 012-04 s2012Joyce RoguinNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- PE (Module 3)Document3 pagesPE (Module 3)angeline medalloNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- ECTDocument11 pagesECTmanu sethi75% (4)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Unit 4 Pain AssessmentDocument5 pagesUnit 4 Pain AssessmentAdellia ZahwaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Drug and Alcohol Awareness ClassDocument71 pagesDrug and Alcohol Awareness ClassRinkish DalliahNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Methodological Issues in Patient Satisfaction SurveyDocument6 pagesMethodological Issues in Patient Satisfaction SurveyLim LeePingNo ratings yet
- Chapter 3 Pediatric Ophthalmology and Orthoptics Pediatric Ophthalmology (PDFDrive)Document202 pagesChapter 3 Pediatric Ophthalmology and Orthoptics Pediatric Ophthalmology (PDFDrive)Johannes UmbohNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Theory of Chronic SorrowDocument13 pagesTheory of Chronic Sorrowrusni rockabilly0% (1)
- Plica PDFDocument7 pagesPlica PDFIVAN VERGARANo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Social Media Impact On Teens Issue Exploration Essay EnglishDocument4 pagesSocial Media Impact On Teens Issue Exploration Essay Englishapi-534589457No ratings yet
- Module 3 Nursing Skills Procedure On GI, Endo-Metab Concept (B)Document19 pagesModule 3 Nursing Skills Procedure On GI, Endo-Metab Concept (B)Nashebah A. BatuganNo ratings yet
- Certificate: DIABETIC PATIENTS OF BHAGALPUR" Under The Supervision of Prof. DRDocument38 pagesCertificate: DIABETIC PATIENTS OF BHAGALPUR" Under The Supervision of Prof. DRsaloniNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Tumor Necrosis Factor Inhibitors in Patients With Takayasu Arteritis: Experience From A Referral Center With Long-Term FollowupDocument5 pagesTumor Necrosis Factor Inhibitors in Patients With Takayasu Arteritis: Experience From A Referral Center With Long-Term FollowupMikhail PisarevNo ratings yet
- Professionalism in Healthcare Professionals: Research ReportDocument68 pagesProfessionalism in Healthcare Professionals: Research ReportSueNo ratings yet
- Abstract Comparison Between Albendazole and MebendazoleDocument25 pagesAbstract Comparison Between Albendazole and MebendazoleluzNo ratings yet
- Inclusive Short NoteDocument80 pagesInclusive Short NoteIyasu taresa100% (1)
- WHO - Creating A Framework Enabling - Healthcare Access For Migrants in Conflict Zones.Document9 pagesWHO - Creating A Framework Enabling - Healthcare Access For Migrants in Conflict Zones.Dhruv AgarwalNo ratings yet
- CHN Midterm Exam CoverageDocument6 pagesCHN Midterm Exam CoverageRoshin Tejero100% (1)
- DR Manavita Mahajan MD (PGI Chandigarh), FRCOG (London) SR Consultant Obstetrician & GynecologistDocument21 pagesDR Manavita Mahajan MD (PGI Chandigarh), FRCOG (London) SR Consultant Obstetrician & Gynecologistﻣﻠﻚ عيسىNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Medical Residency Personal Statement Dissected Sample1Document4 pagesMedical Residency Personal Statement Dissected Sample1Gurkanwal Singh100% (2)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)