You might also like
- Fetal Heart Defects and Measures of Cerebral Size: Objectives Study DesignDocument8 pagesFetal Heart Defects and Measures of Cerebral Size: Objectives Study DesignAdrian KhomanNo ratings yet
- 10 1002@ppul 1950160309 PDFDocument13 pages10 1002@ppul 1950160309 PDFAdrian KhomanNo ratings yet
- Chronic Lung Disease in Premature BabiesDocument2 pagesChronic Lung Disease in Premature BabiesAdrian KhomanNo ratings yet
- BLT 15 259Document9 pagesBLT 15 259Adrian KhomanNo ratings yet
- Danne 2018Document54 pagesDanne 2018Adrian KhomanNo ratings yet
- Chronic Lung Disease in Premature BabiesDocument2 pagesChronic Lung Disease in Premature BabiesAdrian KhomanNo ratings yet
- Jurnal Neuroo Wanigasinghe2015Document7 pagesJurnal Neuroo Wanigasinghe2015melly adityaNo ratings yet
- Be Rent Sen 2015Document12 pagesBe Rent Sen 2015Adrian KhomanNo ratings yet
- DHF Menurut WHO 2011Document212 pagesDHF Menurut WHO 2011Jamal SutrisnaNo ratings yet
- Kugelman2007 PDFDocument7 pagesKugelman2007 PDFAdrian KhomanNo ratings yet
- Merrill 2004Document9 pagesMerrill 2004Adrian KhomanNo ratings yet
- Be Rent Sen 2015Document12 pagesBe Rent Sen 2015Adrian KhomanNo ratings yet
- Miaoying Zhang, Xiaojing Li, Li Xi, Zhuhui Zhao, Ruoqian Cheng, Bingbing Wu and Feihong LuoDocument1 pageMiaoying Zhang, Xiaojing Li, Li Xi, Zhuhui Zhao, Ruoqian Cheng, Bingbing Wu and Feihong LuoAdrian KhomanNo ratings yet
- Jae 201174012905Document5 pagesJae 201174012905Adrian KhomanNo ratings yet
- Practical Algorithms in Pediatric Hematology and OncologyDocument119 pagesPractical Algorithms in Pediatric Hematology and OncologyNubia Ahumadaa100% (5)
- United States Patent (19) 11 Patent Number: 5,969,606: Reber Et Al. (45) Date of Patent: Oct. 19, 1999Document12 pagesUnited States Patent (19) 11 Patent Number: 5,969,606: Reber Et Al. (45) Date of Patent: Oct. 19, 1999Adrian KhomanNo ratings yet
- New Newstart 2Document1 pageNew Newstart 2Adrian KhomanNo ratings yet
- Alan Sari 2016Document11 pagesAlan Sari 2016Adrian KhomanNo ratings yet
- Ehz 467Document65 pagesEhz 467Coy Calapatia-TorresNo ratings yet
- Status Nutrisi WHO Laki-LakiDocument1 pageStatus Nutrisi WHO Laki-LakiAdrian KhomanNo ratings yet
- Treatment of Autoimmune Hemolytic Anemias, 2014 ReviewDocument8 pagesTreatment of Autoimmune Hemolytic Anemias, 2014 ReviewSabina UlubeanuNo ratings yet
- Pocket Pediatrics Handbook for Children by MGHDocument5 pagesPocket Pediatrics Handbook for Children by MGHAdrian KhomanNo ratings yet
- Pediatric Cardiology: Original ArticlesDocument5 pagesPediatric Cardiology: Original ArticlesAdrian KhomanNo ratings yet
- Hemodynamic Study: O Content (mL/100 ML) HB × 1.36 × (O Sat/100)Document9 pagesHemodynamic Study: O Content (mL/100 ML) HB × 1.36 × (O Sat/100)Adrian KhomanNo ratings yet
- Treatment of Autoimmune Hemolytic Anemias, 2014 ReviewDocument8 pagesTreatment of Autoimmune Hemolytic Anemias, 2014 ReviewSabina UlubeanuNo ratings yet
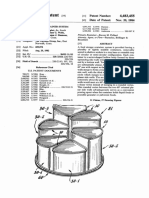
- Food storage container system patentDocument13 pagesFood storage container system patentAdrian KhomanNo ratings yet
- Diagnostic and Therapeutic Challenges of Primary Autoimmune Haemolytic Anaemia in ChildrenDocument7 pagesDiagnostic and Therapeutic Challenges of Primary Autoimmune Haemolytic Anaemia in ChildrenAdrian KhomanNo ratings yet
- Breastfeeding Rates and Programs in Europe: A Survey of 11 National Breastfeeding Committees and RepresentativesDocument8 pagesBreastfeeding Rates and Programs in Europe: A Survey of 11 National Breastfeeding Committees and RepresentativesAdrian KhomanNo ratings yet
- United States Patent (19) 11 Patent Number: 5,969,606: Reber Et Al. (45) Date of Patent: Oct. 19, 1999Document12 pagesUnited States Patent (19) 11 Patent Number: 5,969,606: Reber Et Al. (45) Date of Patent: Oct. 19, 1999Adrian KhomanNo ratings yet
- Pediatric Neurology: Hye-Ryun Yeh MD, Min-Jee Kim MD, Tae-Sung Ko MD, PHD, Mi-Sun Yum MD, PHD, Su-Jeong You MD, PHDDocument6 pagesPediatric Neurology: Hye-Ryun Yeh MD, Min-Jee Kim MD, Tae-Sung Ko MD, PHD, Mi-Sun Yum MD, PHD, Su-Jeong You MD, PHDAdrian KhomanNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Lesson 1 Intellectual Revelations That Define Society: ST ND RDDocument5 pagesLesson 1 Intellectual Revelations That Define Society: ST ND RDEmma Elarde100% (1)
- Atom Infant Incubator Model V-2200: Operation ManualDocument104 pagesAtom Infant Incubator Model V-2200: Operation ManualnagaganasNo ratings yet
- Dara Brodsky MD, Mary Ann Ouellette MS APRN IBCLC-Primary Care of The Premature Infant (2007)Document312 pagesDara Brodsky MD, Mary Ann Ouellette MS APRN IBCLC-Primary Care of The Premature Infant (2007)Hisham Elkilaney100% (1)
- UntitledDocument20 pagesUntitledpratapekkaNo ratings yet
- District Report and Tabulation for PRC Study on Rapid Appraisal of RHM MaduraiDocument108 pagesDistrict Report and Tabulation for PRC Study on Rapid Appraisal of RHM Maduraivelxerox4123No ratings yet
- Pediatrics PDFDocument33 pagesPediatrics PDFChellapandyaNo ratings yet
- Transient Tachypnea of The NewbornDocument2 pagesTransient Tachypnea of The Newbornjulesubayubay5428No ratings yet
- Yuni Santos2017Document8 pagesYuni Santos2017Mastifa HanasitaNo ratings yet
- Causes and Outcomes of Respiratory Distress in NeonatesDocument8 pagesCauses and Outcomes of Respiratory Distress in NeonatesMohammad AlmuhaiminNo ratings yet
- Airborne 185A+ Infant Transport Incubator - ENDocument2 pagesAirborne 185A+ Infant Transport Incubator - ENA. A.G.No ratings yet
- OT - Neonatal - Intensive - Care - IJOT - ENDocument6 pagesOT - Neonatal - Intensive - Care - IJOT - ENSara Gomes CastroNo ratings yet
- Rwanda NeoLENS 15feb2022Document38 pagesRwanda NeoLENS 15feb2022Fachmi Putera Susila SinuratNo ratings yet
- Care of Child With IncubatorDocument26 pagesCare of Child With IncubatorSabita Paudel100% (2)
- Congenital Diaphragmatic Hernias (CDH)Document24 pagesCongenital Diaphragmatic Hernias (CDH)tsega tilahunNo ratings yet
- Massage Improves Weight Gain in Preterm InfantsDocument6 pagesMassage Improves Weight Gain in Preterm Infantsari dwiNo ratings yet
- NCLEX Questions - OB MATERNITY QUESTIONS PDFDocument17 pagesNCLEX Questions - OB MATERNITY QUESTIONS PDFAnneRaquelTalentoNo ratings yet
- EINC - A Step-By-Step Guide FinalDocument40 pagesEINC - A Step-By-Step Guide FinalAnonymous h2EnKyDbNo ratings yet
- DSC BookDocument52 pagesDSC BookPriti Khemka60% (5)
- Mentor Interview Questions TemplateDocument3 pagesMentor Interview Questions Templateapi-377526885No ratings yet
- Giraffe OmniBed Carestation BrochureDocument7 pagesGiraffe OmniBed Carestation BrochureMohd Khidir GazaliNo ratings yet
- Erica Anacleto ResumeDocument3 pagesErica Anacleto Resumeapi-282272358No ratings yet
- Curr Vitae DR EkoDocument3 pagesCurr Vitae DR EkoFaisallrizzaNo ratings yet
- Updated ResumeDocument5 pagesUpdated ResumeMaJoy Oxen Dali-oneNo ratings yet
- Guia Basada en La Evidencia Canguro 2019Document8 pagesGuia Basada en La Evidencia Canguro 2019luzhelanapaezNo ratings yet
- SNCU Process in Madhya Pradesh NIPI DistrictsDocument7 pagesSNCU Process in Madhya Pradesh NIPI DistrictsDr Rajan Dubey100% (1)
- EPC FAC Guide pt2 Mod 1N 7N PDFDocument123 pagesEPC FAC Guide pt2 Mod 1N 7N PDFmaxamaxaNo ratings yet
- IncubatorsDocument4 pagesIncubatorsKarjana183No ratings yet
- Clarifications Facilities Items v5Document17 pagesClarifications Facilities Items v5HundalHarmanNo ratings yet
- Pediatric Neuroimaging (PDFDrive)Document1,708 pagesPediatric Neuroimaging (PDFDrive)Roberto Duni100% (1)