You might also like
- ACLS Test BankDocument13 pagesACLS Test BankSofiaSheikh94% (51)
- Pediatric Mock Resuscitation ScenariosDocument6 pagesPediatric Mock Resuscitation ScenariosdinkytinkNo ratings yet
- Pepp Als PretestDocument4 pagesPepp Als PretestDave BoppNo ratings yet
- Defibrillation - E-Learning Quiz 1. Identify The RhythmDocument3 pagesDefibrillation - E-Learning Quiz 1. Identify The RhythmBalaji Chinnasami100% (1)
- Cals ReviewbjvjvjDocument14 pagesCals ReviewbjvjvjCarl Jay M Ocariza100% (1)
- 2010 Integrated Updated Circulation ACLS Acute Coronary Syndromes AlgorithmDocument1 page2010 Integrated Updated Circulation ACLS Acute Coronary Syndromes Algorithmms_lezahNo ratings yet
- ACLS Appendix 3Document32 pagesACLS Appendix 3tostc100% (1)
- AHA ELearning ACLS Precourse Self-Assessment and Precourse WorkDocument1 pageAHA ELearning ACLS Precourse Self-Assessment and Precourse Work9kjsntkrzcNo ratings yet
- Acls Study Guide 2016Document2 pagesAcls Study Guide 2016nova939100% (2)
- AHA PALS Core Case Test ChecklistsDocument12 pagesAHA PALS Core Case Test ChecklistsVitor Hugo G CorreiaNo ratings yet
- PALS Case Scenario Testing ChecklistDocument12 pagesPALS Case Scenario Testing ChecklistJohn David D. ErguizaNo ratings yet
- Summary of High-Quality CPR Components For BLS ProvidersDocument1 pageSummary of High-Quality CPR Components For BLS ProvidersPhilippe Ceasar C. BascoNo ratings yet
- Picmonic Glycogen Storage DiseasesDocument2 pagesPicmonic Glycogen Storage DiseasesLaylee Clare100% (3)
- ICF-CY Developmental Code Sets CHECKLIST 6-12Document3 pagesICF-CY Developmental Code Sets CHECKLIST 6-12Clau Miranda Mendoza100% (1)
- Cardiac Rehabilitation GuidelineDocument57 pagesCardiac Rehabilitation GuidelineCarolina Pereira100% (1)
- Learning Cardiac Auscultation by Taylor and Springer From Am MedicalbooksDocument327 pagesLearning Cardiac Auscultation by Taylor and Springer From Am MedicalbooksSivakumar Gounden100% (1)
- Complete Revision Notes by Vincent Helyar and Aidan Shaw 2018Document645 pagesComplete Revision Notes by Vincent Helyar and Aidan Shaw 2018Zubair Lone100% (4)
- AHA ACLS Written Test: Ready To Study? Start With FlashcardsDocument8 pagesAHA ACLS Written Test: Ready To Study? Start With FlashcardssallyNo ratings yet
- ACLS Rhythms Cheat Sheet PDFDocument21 pagesACLS Rhythms Cheat Sheet PDFNavin ShawnNo ratings yet
- 3 Combined AHA BLS ACLS Updates CombinedDocument5 pages3 Combined AHA BLS ACLS Updates Combinedamanrup randhawa100% (1)
- BLS Answer SheetDocument1 pageBLS Answer SheetGenesis SarengoNo ratings yet
- Normal Ranges Vital Signs 2017Document2 pagesNormal Ranges Vital Signs 2017Elvis Nguyen100% (1)
- Pals Life SaverDocument13 pagesPals Life SaverStephany ZamorasNo ratings yet
- Emergency Nursing: Roles of Emergency NurseDocument6 pagesEmergency Nursing: Roles of Emergency NursejorgeacctNo ratings yet
- Acls Review 2015Document29 pagesAcls Review 2015JB Reyes100% (2)
- BLS Study Guide and Pretest PrintableDocument13 pagesBLS Study Guide and Pretest PrintableSkill Lab0% (1)
- ACLS PresentationDocument79 pagesACLS PresentationHumaira YasserNo ratings yet
- BLS MCQDocument8 pagesBLS MCQAmit BhowmikNo ratings yet
- ACLS Precourse Self-AssessmentDocument2 pagesACLS Precourse Self-AssessmentMandela KibiritiNo ratings yet
- Bls Study GuideDocument2 pagesBls Study GuideJohnNo ratings yet
- BLS & AclsDocument13 pagesBLS & AclsadamNo ratings yet
- ACLS Study GuideDocument30 pagesACLS Study GuidemmmmzNo ratings yet
- ACLS Instr Fac GuideDocument43 pagesACLS Instr Fac GuideOnek KothaNo ratings yet
- ACLS Pre Course Package 2015 BC ActiveDocument40 pagesACLS Pre Course Package 2015 BC ActiverousbekNo ratings yet
- 15 Item Acls DrillDocument4 pages15 Item Acls DrillVal SolidumNo ratings yet
- Shengwang-Job Portfolio Zuizhongban 1Document7 pagesShengwang-Job Portfolio Zuizhongban 1api-505043323No ratings yet
- ACLS Practical Case Scenarios (1 June 2011)Document15 pagesACLS Practical Case Scenarios (1 June 2011)nersNo ratings yet
- Cardiac RehabilitationDocument37 pagesCardiac RehabilitationNafees AsgharNo ratings yet
- ACLS Skills ChecklistDocument2 pagesACLS Skills ChecklistKary ParraNo ratings yet
- ACLS Skills ChecklistDocument2 pagesACLS Skills ChecklistMuhammad Zubair100% (1)
- Pediatric FirstAid CPR AEDDocument12 pagesPediatric FirstAid CPR AEDVirtuepearlsNo ratings yet
- Introd To ECG Code Blue Champs March 2019Document52 pagesIntrod To ECG Code Blue Champs March 2019james rukenya100% (1)
- Aha Acls Prep Packet 2020Document69 pagesAha Acls Prep Packet 2020VP The Hacker100% (2)
- ACLS Study Guide: Ecg Strip InterpretationDocument12 pagesACLS Study Guide: Ecg Strip InterpretationMariana Berger100% (1)
- Megacode Testing Checklist Scenarios 4-7-10 Tachycardia, VF, PEA, PC...Document1 pageMegacode Testing Checklist Scenarios 4-7-10 Tachycardia, VF, PEA, PC...krgduraiNo ratings yet
- Pals CardDocument12 pagesPals CardSara KhanNo ratings yet
- LSCPR Pals Study Guide 2020Document57 pagesLSCPR Pals Study Guide 2020Juan Ma100% (1)
- Assessment Algorithm For Sedated Adult ICU Patients: No YesDocument18 pagesAssessment Algorithm For Sedated Adult ICU Patients: No YeshendraNo ratings yet
- Adult Post-Cardiac Arrest Care Algorithm: o Co Io o CoDocument1 pageAdult Post-Cardiac Arrest Care Algorithm: o Co Io o CoKavya ShreeNo ratings yet
- Shock: Shout For Help/Activate Emergency ResponseDocument6 pagesShock: Shout For Help/Activate Emergency ResponseandiyanimalikNo ratings yet
- Chest Pain: Jean J. Chatham, MDDocument40 pagesChest Pain: Jean J. Chatham, MDYermia RashaquatNo ratings yet
- AclsDocument11 pagesAclsdyah rahayu hutamiNo ratings yet
- The Six Second ECGDocument9 pagesThe Six Second ECGAC0RNNo ratings yet
- AclsDocument85 pagesAclsJulia CostaNo ratings yet
- Dysrhythmia Advance Content Outline A1 - 2020.1.2Document3 pagesDysrhythmia Advance Content Outline A1 - 2020.1.2Kimberly Whiteside50% (2)
- ICU Drips: Stephanie Sanderson, RN, MSN, CNS, CCNS, CCRN Medical Cardiac ICU-UNMHDocument32 pagesICU Drips: Stephanie Sanderson, RN, MSN, CNS, CCNS, CCRN Medical Cardiac ICU-UNMHNicole Adkins100% (1)
- PALS Precourse Self 2023Document9 pagesPALS Precourse Self 2023Airene SibleNo ratings yet
- Aha Acls Prep Packet 2021 NewDocument69 pagesAha Acls Prep Packet 2021 Newdim100% (2)
- Cns Stimulants: Drug Name Class Uses Action Side EffectsDocument6 pagesCns Stimulants: Drug Name Class Uses Action Side EffectsJennifer ViciosoNo ratings yet
- 1 AlgorithmsDocument19 pages1 AlgorithmsRiya Sood100% (1)
- Dysrhythmia TestsDocument3 pagesDysrhythmia TestsKimberly WhitesideNo ratings yet
- Acute Medical Emergencies: The Practical ApproachFrom EverandAcute Medical Emergencies: The Practical ApproachNo ratings yet
- Mitral Valve Regurgitation, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandMitral Valve Regurgitation, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Patient Throughput And Capacity Management A Complete Guide - 2020 EditionFrom EverandPatient Throughput And Capacity Management A Complete Guide - 2020 EditionNo ratings yet
- Microbiology Made Ludicrously Simpler1!!!Document59 pagesMicrobiology Made Ludicrously Simpler1!!!Laylee Clare100% (2)
- Society For Education in Anesthesia Medical Student Guide To Anesthesiology Fifth Edition 2009Document46 pagesSociety For Education in Anesthesia Medical Student Guide To Anesthesiology Fifth Edition 2009Laylee ClareNo ratings yet
- GIA 2nd Edition - PDFDocument22 pagesGIA 2nd Edition - PDFLaylee ClareNo ratings yet
- HIV AIDS Opportunistic InfectionsDocument26 pagesHIV AIDS Opportunistic InfectionsLaylee ClareNo ratings yet
- Mind Map - FatigueDocument1 pageMind Map - FatigueLaylee ClareNo ratings yet
- Surgery Case 3Document2 pagesSurgery Case 3Laylee ClareNo ratings yet
- Antimicrobial Drugs TableDocument19 pagesAntimicrobial Drugs TableLaylee ClareNo ratings yet
- Roadmap To Residency 2017Document51 pagesRoadmap To Residency 2017Laylee ClareNo ratings yet
- Roadmap To Residency 2017Document51 pagesRoadmap To Residency 2017Laylee ClareNo ratings yet
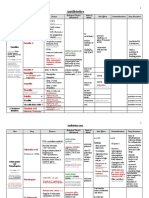
- AntibioticDocument4 pagesAntibioticionanic72No ratings yet
- Diuretics TableDocument5 pagesDiuretics TableLaylee ClareNo ratings yet
- Most Comon Questions Asked in NEET PG and DNBDocument12 pagesMost Comon Questions Asked in NEET PG and DNBSubhajitPaul100% (2)
- Daftar Singkatan KardioDocument1 pageDaftar Singkatan KardioIb WiadnyanaNo ratings yet
- ESP AssignmentDocument15 pagesESP AssignmentPhúc Đoàn0% (2)
- SureFire CPR NRP Study GuideDocument18 pagesSureFire CPR NRP Study GuidelykaNo ratings yet
- Ajr 16 16449Document9 pagesAjr 16 16449Lbc CruzNo ratings yet
- Jurnal The Heart and Cardiovascular System in The Qur'An and HadeethDocument19 pagesJurnal The Heart and Cardiovascular System in The Qur'An and HadeethWidya Derattano Pikal LimNo ratings yet
- Pulmonary Arterial Hypertension Pathogenesis and Clinical ManagementDocument27 pagesPulmonary Arterial Hypertension Pathogenesis and Clinical ManagementMr. LNo ratings yet
- Drowning PDFDocument7 pagesDrowning PDFAditya Chandra ForestaNo ratings yet
- EECP Clinical ResultsDocument44 pagesEECP Clinical ResultsAryadhi TevataqsaNo ratings yet
- Congestive Heart FailureDocument6 pagesCongestive Heart Failureseigelystic100% (1)
- New Patients EndocarditisDocument1 pageNew Patients EndocarditisnayanastarNo ratings yet
- 080 - Hospital Information Document For New StaffDocument2 pages080 - Hospital Information Document For New StaffleicesterbugNo ratings yet
- Cardiac Morphology and Function of Hyperthyroid Patients Admitted at de La Salle University Medical CenterDocument7 pagesCardiac Morphology and Function of Hyperthyroid Patients Admitted at de La Salle University Medical CenterSamej NaviNo ratings yet
- Absite Review QuestionsDocument81 pagesAbsite Review QuestionsJames JosephNo ratings yet
- NewCardio, Inc.Document2 pagesNewCardio, Inc.MattNo ratings yet
- NCP For HypertensionDocument6 pagesNCP For HypertensionJaic Ealston D. Tampus0% (2)
- Curs Ic - Ic Si Ci - Final - 11 - Nov 2013Document675 pagesCurs Ic - Ic Si Ci - Final - 11 - Nov 2013Bogdanel MihaiNo ratings yet
- Acls 11Document13 pagesAcls 11ezzat salemNo ratings yet
- Kr2med 2006engDocument62 pagesKr2med 2006engHind YousifNo ratings yet
- July 6 CXC BiologyDocument73 pagesJuly 6 CXC BiologyShantay BurtonNo ratings yet
- Cvs ExaminationDocument3 pagesCvs ExaminationJared Khoo Er HauNo ratings yet
- Physical Fitness AssessmentDocument30 pagesPhysical Fitness AssessmentJingle BellsNo ratings yet
- Intra Aortic Balloon Pump (IABP) 2009Document57 pagesIntra Aortic Balloon Pump (IABP) 2009nurminsyahNo ratings yet
- Journal Bedah Thorax 2Document15 pagesJournal Bedah Thorax 2Novia LarasatiNo ratings yet
- Varicose Veins Treatment and Prognosis in Ayurveda Ascompared To ModernDocument3 pagesVaricose Veins Treatment and Prognosis in Ayurveda Ascompared To ModernEditor IJTSRDNo ratings yet
- NMS Surgery Casebook CH 1 Preoperative Care Flashcards - ProProfsDocument3 pagesNMS Surgery Casebook CH 1 Preoperative Care Flashcards - ProProfsWade Bullock0% (1)