You might also like
- Dim Light Melatonin Onset (DLMO) A Tool For The Analysis of Circadian Phase in Human Sleep and Chronobiological DisordersDocument11 pagesDim Light Melatonin Onset (DLMO) A Tool For The Analysis of Circadian Phase in Human Sleep and Chronobiological DisordersMarko PotočnikNo ratings yet
- In Uence of Light Intensity, Spectrum and Orientation On Sea Bass Plasma and Ocular MelatoninDocument7 pagesIn Uence of Light Intensity, Spectrum and Orientation On Sea Bass Plasma and Ocular MelatoninMarko PotočnikNo ratings yet
- Suppression of Melatonin Secretion in Some Blind Patients by Exposure To Bright LightDocument6 pagesSuppression of Melatonin Secretion in Some Blind Patients by Exposure To Bright LightMarko PotočnikNo ratings yet
- The Influence of Different Light Spectra On The Suppression of Pineal Melatonin Content in The Syrian HamsterDocument7 pagesThe Influence of Different Light Spectra On The Suppression of Pineal Melatonin Content in The Syrian HamsterMarko PotočnikNo ratings yet
- An Action Spectrum For Melatonin Suppression Evidence For A Novel Non-Rod, Non-Cone Photoreceptor System in HumansDocument7 pagesAn Action Spectrum For Melatonin Suppression Evidence For A Novel Non-Rod, Non-Cone Photoreceptor System in HumansMarko PotočnikNo ratings yet
- Suppression of Melatonin Secretion in Some Blind Patients by Exposure To Bright LightDocument6 pagesSuppression of Melatonin Secretion in Some Blind Patients by Exposure To Bright LightMarko PotočnikNo ratings yet
- Blue Light From Light-Emitting Diodes Elicits A Dose-Dependent Suppression of Melatonin in HumansDocument5 pagesBlue Light From Light-Emitting Diodes Elicits A Dose-Dependent Suppression of Melatonin in HumansMarko PotočnikNo ratings yet
- Light Level and Duration of Exposure Determine The Impact of Self-Luminous Tablets On Melatonin SuppressionDocument4 pagesLight Level and Duration of Exposure Determine The Impact of Self-Luminous Tablets On Melatonin SuppressionMarko PotočnikNo ratings yet
- Sensitivity of The Human Circadian Pacemaker To Nocturnal Light Melatonin Phase Resetting and SuppressionDocument8 pagesSensitivity of The Human Circadian Pacemaker To Nocturnal Light Melatonin Phase Resetting and SuppressionMarko PotočnikNo ratings yet
- Blue Blocker Glasses Impede The Capacity of Bright Light To Suppress Melatonin ProductionDocument6 pagesBlue Blocker Glasses Impede The Capacity of Bright Light To Suppress Melatonin ProductionMarko PotočnikNo ratings yet
- 10 1176@ajp 142 6 725Document3 pages10 1176@ajp 142 6 725Marko PotočnikNo ratings yet
- Light Suppresses Melatonm Secretion in HumansDocument3 pagesLight Suppresses Melatonm Secretion in HumansMarko PotočnikNo ratings yet
- Melatonin Saliva CollectionDocument1 pageMelatonin Saliva CollectionMarko PotočnikNo ratings yet
- Lewy 1989Document10 pagesLewy 1989Marko PotočnikNo ratings yet
- Lewy 1983Document6 pagesLewy 1983Marko PotočnikNo ratings yet
- TEMT6000Document6 pagesTEMT6000Alph Sieg KettenwulfNo ratings yet
- Zats 1988Document12 pagesZats 1988Marko PotočnikNo ratings yet
- Cahill 1996Document5 pagesCahill 1996Marko PotočnikNo ratings yet
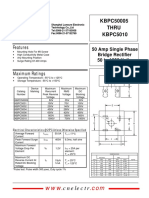
- KBPC50005 thru KBPC5010 50 Amp Single Phase Bridge Rectifier Features and SpecificationsDocument2 pagesKBPC50005 thru KBPC5010 50 Amp Single Phase Bridge Rectifier Features and SpecificationsMarko PotočnikNo ratings yet
- Zatz 1989Document5 pagesZatz 1989Marko PotočnikNo ratings yet
- Ipadio0010032 PDFDocument2 pagesIpadio0010032 PDFMarko PotočnikNo ratings yet
- 3 Protective Treatment of Aluminum and Its AlloysDocument5 pages3 Protective Treatment of Aluminum and Its AlloysMarko PotočnikNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- CP PPTDocument58 pagesCP PPTKatherine 'Chingboo' Leonico LaudNo ratings yet
- IRBD Scales Abnormal Involuntary Movement ScaleDocument2 pagesIRBD Scales Abnormal Involuntary Movement ScaleRoberto LlanesNo ratings yet
- PCAP - SummaryDocument4 pagesPCAP - SummaryNani TumlosNo ratings yet
- Types of ArrhythmiaDocument10 pagesTypes of ArrhythmiaRonilyn Mae AlvarezNo ratings yet
- Cyclosporine PharmaDocument2 pagesCyclosporine PharmaflagaacNo ratings yet
- Heti 2021 IPPE POSTER VOLTEIODocument1 pageHeti 2021 IPPE POSTER VOLTEIOAline SartiNo ratings yet
- HEALTHY TITLEDocument10 pagesHEALTHY TITLEermal_binoNo ratings yet
- Chronic Renal FailureDocument54 pagesChronic Renal FailureAkia Cayasan BayaNo ratings yet
- The many benefits of music. Listening to and creating music helps children learn numeracy, literacy and emotional skillsDocument5 pagesThe many benefits of music. Listening to and creating music helps children learn numeracy, literacy and emotional skillsHarold JimenezNo ratings yet
- Administration Unit AccommodationDocument134 pagesAdministration Unit AccommodationAdil AbdoNo ratings yet
- What Are Anxiety Disorder/depression?Document4 pagesWhat Are Anxiety Disorder/depression?Joanna Mæ Nuñez SaysønNo ratings yet
- Rheumatic Heart Disease Causes, Symptoms, and TreatmentDocument4 pagesRheumatic Heart Disease Causes, Symptoms, and TreatmentJhen Jhen100% (1)
- Mental Health Nursing Exam QuestionsDocument17 pagesMental Health Nursing Exam QuestionsSubiVictorNo ratings yet
- An A Boli ZantesDocument3 pagesAn A Boli Zantesvinigoncalves275No ratings yet
- Program - ICU Rehab 2023Document7 pagesProgram - ICU Rehab 2023Ronni Untung HNo ratings yet
- Carl Rogers (1902-1987) : Humanistic-Existential Paradigm Self TheoryDocument22 pagesCarl Rogers (1902-1987) : Humanistic-Existential Paradigm Self TheoryRhaine EstebanNo ratings yet
- Counselling Process - TYBA Psychology HonorsDocument12 pagesCounselling Process - TYBA Psychology HonorsP K Tunn100% (1)
- Annotated Bibliography ProjectDocument6 pagesAnnotated Bibliography Projectapi-237649440No ratings yet
- Clinical Audit: Pain Management in Total Knee Replacement Aadhar Hospital January - July 2018Document29 pagesClinical Audit: Pain Management in Total Knee Replacement Aadhar Hospital January - July 2018Relacy Healthcare100% (2)
- Heart Failure Nursing InterventionsDocument301 pagesHeart Failure Nursing Interventionsticoystephanie100% (2)
- Labor and Delivery QuizDocument7 pagesLabor and Delivery QuizAmy50% (2)
- 14 Cancer Symptoms Women Ignore - 3Document1 page14 Cancer Symptoms Women Ignore - 3Meidi RaniNo ratings yet
- Protein TherapeuticsDocument14 pagesProtein TherapeuticsSumanth Kumar ReddyNo ratings yet
- GFCH Travel FormulasDocument2 pagesGFCH Travel FormulasWilliam TellNo ratings yet
- Terapia de Fluor AAPDDocument4 pagesTerapia de Fluor AAPDAndy HerreraNo ratings yet
- Androgenetic AlopeciaDocument22 pagesAndrogenetic AlopeciaYuliannisa Nyunyun100% (1)
- Freedom at Your FingertipsDocument30 pagesFreedom at Your FingertipsLucian Grec100% (1)
- Hyperglycemic CrisisDocument9 pagesHyperglycemic CrisisRoberto López MataNo ratings yet
- Active ListeningDocument6 pagesActive ListeningQumail RazaNo ratings yet
- ClonazepamDocument2 pagesClonazepamjhezelle05100% (2)