You might also like
- Business Statistics: Fourth Canadian EditionDocument41 pagesBusiness Statistics: Fourth Canadian EditionTaron AhsanNo ratings yet
- Citroen CX Manual Series 2 PDFDocument646 pagesCitroen CX Manual Series 2 PDFFilipe Alberto Magalhaes0% (1)
- Design of Ultra Deep Water Rigid & Flexible Pipelay/ Heavy Lift/ DP3 Construction VesselDocument33 pagesDesign of Ultra Deep Water Rigid & Flexible Pipelay/ Heavy Lift/ DP3 Construction VesselNAV KOL100% (1)
- Hoc3 CatalogoDocument12 pagesHoc3 CatalogoChristianReinoso0% (1)
- QBase Anaesthesia 1Document209 pagesQBase Anaesthesia 1Sanj.etcNo ratings yet
- The Basic Anaesthesia Machine: Review ArticleDocument14 pagesThe Basic Anaesthesia Machine: Review Articlewahyuwirawan100% (1)
- Anaesthesia Machine LectureDocument99 pagesAnaesthesia Machine LectureVithal DhulkhedNo ratings yet
- The Basic Anaesthesia MachineDocument13 pagesThe Basic Anaesthesia MachineprasadrottiNo ratings yet
- Digital 20293676 S Nurul FebriantiDocument8 pagesDigital 20293676 S Nurul FebriantiMuhammadIlhamNo ratings yet
- 1 s2.0 S0263876203723685 Main PDFDocument40 pages1 s2.0 S0263876203723685 Main PDFrishikeshmandawadNo ratings yet
- Status of The Ring RF Systems For FairDocument3 pagesStatus of The Ring RF Systems For Fairtanmoy bhattacharjeeNo ratings yet
- Ijert Ijert: Effect of Wind Load On Pressure Vessel Design by Using Non-Linear Finite Element Analysis (FEA)Document7 pagesIjert Ijert: Effect of Wind Load On Pressure Vessel Design by Using Non-Linear Finite Element Analysis (FEA)Jitender SainiNo ratings yet
- T5pg1 6Document6 pagesT5pg1 6ramsebNo ratings yet
- Power Sources For Autonomous Underwater Vehicles: Øistein Hasvold, Nils J. Størkersen, Sissel Forseth, Torleif LianDocument8 pagesPower Sources For Autonomous Underwater Vehicles: Øistein Hasvold, Nils J. Størkersen, Sissel Forseth, Torleif LianmspetroNo ratings yet
- Annexure - I (Sealdah)Document7 pagesAnnexure - I (Sealdah)Gurupada SahooNo ratings yet
- Filament Winding - Introduction and Overview: S.T. Peters, Process Research, ConsultantsDocument5 pagesFilament Winding - Introduction and Overview: S.T. Peters, Process Research, Consultantsalst2323No ratings yet
- Clarification 3728891Document2 pagesClarification 3728891sahapallab7059No ratings yet
- 2.8 Environment and Health During Production: Description Value UnitDocument1 page2.8 Environment and Health During Production: Description Value Unitqc_531040655No ratings yet
- A/R 5-401 Office of Emergency Medical Services Administrative Requirements ManualDocument10 pagesA/R 5-401 Office of Emergency Medical Services Administrative Requirements ManualCEMARANo ratings yet
- Spontaneus 3Document6 pagesSpontaneus 3hoanNo ratings yet
- PDF 12349Document2 pagesPDF 12349Cae Fea CfdNo ratings yet
- J Nucengdes 2014 04 031Document13 pagesJ Nucengdes 2014 04 031shivaprabhuNo ratings yet
- Emergency Flare Design Features System-Some Practical: A The TheDocument3 pagesEmergency Flare Design Features System-Some Practical: A The Thekumar_chemicalNo ratings yet
- Nitrogen Tank Blanketing 0415Document4 pagesNitrogen Tank Blanketing 0415NursahidNo ratings yet
- Hydromechanics Characterization of The Turbulent Flow Generated by Anchor ImpellersDocument15 pagesHydromechanics Characterization of The Turbulent Flow Generated by Anchor ImpellersoussemaNo ratings yet
- US6415860Document18 pagesUS6415860babithyNo ratings yet
- Vibration Analysis in Reciprocating CompressorsDocument11 pagesVibration Analysis in Reciprocating Compressorsakamalapuri388No ratings yet
- SPE 10255 Sucker Rod Pumping Systems Design - Another Look: by Paul M. Bommer, Bommer Engineering CoDocument1 pageSPE 10255 Sucker Rod Pumping Systems Design - Another Look: by Paul M. Bommer, Bommer Engineering Coosorio--No ratings yet
- MP2017F - Reveillere CAESnewbeginning v2 PDocument13 pagesMP2017F - Reveillere CAESnewbeginning v2 PAndrea La FiuraNo ratings yet
- automatedShockTube Fuller19Document9 pagesautomatedShockTube Fuller19ennioNo ratings yet
- Section 35 - Air Conditioning and Mechanic Ventilation SystemDocument32 pagesSection 35 - Air Conditioning and Mechanic Ventilation SystemMAYMODERN SITEINFONo ratings yet
- HB 147-2000 Sprinklers SimplifiedDocument10 pagesHB 147-2000 Sprinklers SimplifiedSAI Global - APACNo ratings yet
- Nuclear Engineering and Design: Diego Castelliti, Guglielmo LomonacoDocument12 pagesNuclear Engineering and Design: Diego Castelliti, Guglielmo LomonacoIsma-MANo ratings yet
- EP 1 Final - 082908Document25 pagesEP 1 Final - 082908tuanphamNo ratings yet
- Telemicroscopy Erosion Measurements of 5Document7 pagesTelemicroscopy Erosion Measurements of 5Sanico PrulliNo ratings yet
- Pulverisation and Homogenization of Soil SampleDocument8 pagesPulverisation and Homogenization of Soil SampleWAHEED JUBRILNo ratings yet
- Mat Ing EXAMEN 2 V1Document8 pagesMat Ing EXAMEN 2 V1Richard VillónNo ratings yet
- Design by Analysis According To ASME Section VIII Division 2 For Pump TrapDocument14 pagesDesign by Analysis According To ASME Section VIII Division 2 For Pump TrapSandeep BhatiaNo ratings yet
- Дискурс по сильфонным компенсаторамDocument12 pagesДискурс по сильфонным компенсаторамОлеся ТвиклерNo ratings yet
- Oxygen Concentrators For District Hospitals: Michael B Dobson, John Radcliffe Hospital, Oxford, UKDocument3 pagesOxygen Concentrators For District Hospitals: Michael B Dobson, John Radcliffe Hospital, Oxford, UKAwadhNo ratings yet
- Review of Flow-Through Design in Thermoacoustic RefrigerationDocument5 pagesReview of Flow-Through Design in Thermoacoustic RefrigerationjohnnyNo ratings yet
- Use of Sound Signals in Analyzing Flow Behavior in Steel VesselsDocument10 pagesUse of Sound Signals in Analyzing Flow Behavior in Steel VesselsJJNo ratings yet
- 004 Strain Gage Based TransducersDocument151 pages004 Strain Gage Based TransducersMarcoshhNo ratings yet
- LINK-History of ProtectionDocument7 pagesLINK-History of ProtectionBattinapati ShivaNo ratings yet
- Consideration of Fatigue Life in The Design of Vessels in Molecular Sieve Dryer ServiceDocument9 pagesConsideration of Fatigue Life in The Design of Vessels in Molecular Sieve Dryer Servicevaratharajan g rNo ratings yet
- Crijeneric RefDocument14 pagesCrijeneric RefDidem AcarNo ratings yet
- Modern Integrated Anaesthesia WorkstationDocument9 pagesModern Integrated Anaesthesia WorkstationBryan MaldonadoNo ratings yet
- Traveling Grate Boiler 50 TPH 95 KGCM 450CDocument52 pagesTraveling Grate Boiler 50 TPH 95 KGCM 450CMajid KhanNo ratings yet
- 50 Year History of The Aiche Ammonia Safety Symposium: Gerald P. WilliamsDocument9 pages50 Year History of The Aiche Ammonia Safety Symposium: Gerald P. Williamsvaratharajan g rNo ratings yet
- Adaptive Control of Hot-Dip Galvanizing : PergamonDocument19 pagesAdaptive Control of Hot-Dip Galvanizing : PergamonHerdisNo ratings yet
- Albers 2011Document3 pagesAlbers 2011Ramin ShojaNo ratings yet
- Zero Blow Down Cooling TowerDocument8 pagesZero Blow Down Cooling TowerprakashNo ratings yet
- Is.8188.1999 0 PDFDocument25 pagesIs.8188.1999 0 PDFArunkumar ChandaranNo ratings yet
- Fluid Viscous Dampers of The Izmit Bay Bridge, Turkey Design Requirements and Full-Scale TestingDocument12 pagesFluid Viscous Dampers of The Izmit Bay Bridge, Turkey Design Requirements and Full-Scale TestingSebastian Contreras ContrerasNo ratings yet
- Elektromotoren Und Gerätebau Barleben GMBH: Transformer Protection Relays (Buchholz Principle)Document28 pagesElektromotoren Und Gerätebau Barleben GMBH: Transformer Protection Relays (Buchholz Principle)soltaniNo ratings yet
- Nuclear Safety HistoryDocument26 pagesNuclear Safety HistorycaffiNo ratings yet
- Ija 64 171Document10 pagesIja 64 171little mushroomNo ratings yet
- S.C. Li 1.1 Cavitation: 1.1.1 DiscoveryDocument8 pagesS.C. Li 1.1 Cavitation: 1.1.1 DiscoveryRhonda BushNo ratings yet
- Chemical Micro Process Engineering: Fundamentals, Modelling and ReactionsFrom EverandChemical Micro Process Engineering: Fundamentals, Modelling and ReactionsNo ratings yet
- Exposure Assessment and Safety Considerations for Working with Engineered NanoparticlesFrom EverandExposure Assessment and Safety Considerations for Working with Engineered NanoparticlesNo ratings yet
- Ejectors for Efficient Refrigeration: Design, Applications and Computational Fluid DynamicsFrom EverandEjectors for Efficient Refrigeration: Design, Applications and Computational Fluid DynamicsNo ratings yet
- The Mathematical Understanding of Chemical Engineering SystemsFrom EverandThe Mathematical Understanding of Chemical Engineering SystemsNo ratings yet
- Transfer of The Critically Ill Patient - PACTDocument3 pagesTransfer of The Critically Ill Patient - PACTSanj.etcNo ratings yet
- Foetal AutopsyDocument17 pagesFoetal AutopsySanj.etcNo ratings yet
- 6 - Glossary - PactDocument7 pages6 - Glossary - PactSanj.etcNo ratings yet
- Rhabdomyolysis - PACTDocument2 pagesRhabdomyolysis - PACTSanj.etcNo ratings yet
- Secondary Transport - PactDocument4 pagesSecondary Transport - PactSanj.etcNo ratings yet
- GUIDELINE For IMPROVING OUTCOME After Anaesthesia and Critical Care - 2017 - College of AnaesthesiologistsDocument83 pagesGUIDELINE For IMPROVING OUTCOME After Anaesthesia and Critical Care - 2017 - College of AnaesthesiologistsSanj.etcNo ratings yet
- 500 SBA Gen Systemic Pathology PDFDocument27 pages500 SBA Gen Systemic Pathology PDFSanj.etcNo ratings yet
- Med Oncology MCQDocument109 pagesMed Oncology MCQdrzika100% (8)
- Peripartum Collapse 4.0Document14 pagesPeripartum Collapse 4.0Sanj.etcNo ratings yet
- Opioid and Non-Opioid Analgesics in The ICUDocument2 pagesOpioid and Non-Opioid Analgesics in The ICUSanj.etcNo ratings yet
- SLCoP Sinhala5405694062132472021Document1 pageSLCoP Sinhala5405694062132472021Sanj.etcNo ratings yet
- BMI 8 Selection ExamDocument4 pagesBMI 8 Selection ExamSanj.etcNo ratings yet
- Delirium in Critically IllDocument37 pagesDelirium in Critically IllSanj.etcNo ratings yet
- Gas CylindersDocument9 pagesGas CylindersSanj.etcNo ratings yet
- Intravenous FluidsDocument37 pagesIntravenous FluidsStella UmehNo ratings yet
- Management of Safe AnaesthesiaDocument38 pagesManagement of Safe AnaesthesiaSanj.etcNo ratings yet
- Epidurals and Spinals - Apr16Document6 pagesEpidurals and Spinals - Apr16Sanj.etcNo ratings yet
- Antimicrobial Stewardship Systems and Processes For Effective Antimicrobial Medicine Use PDF 1837273110469Document52 pagesAntimicrobial Stewardship Systems and Processes For Effective Antimicrobial Medicine Use PDF 1837273110469Sanj.etcNo ratings yet
- J Coll Physicians Surg Pak 2014 24 8 603 605Document3 pagesJ Coll Physicians Surg Pak 2014 24 8 603 605Sanj.etcNo ratings yet
- 128 Diabetic KetoacidosisDocument9 pages128 Diabetic KetoacidosisDite Bayu NugrohoNo ratings yet
- A Non-Fatal Self-Poisoning Attempt With Sildenafil: by Guest On 11 November 2017Document5 pagesA Non-Fatal Self-Poisoning Attempt With Sildenafil: by Guest On 11 November 2017Sanj.etcNo ratings yet
- Endgames: Acute EpiglottitisDocument3 pagesEndgames: Acute EpiglottitisSanj.etcNo ratings yet
- Ain ShamsJAnaesthesiol73336 7108132 - 015828Document4 pagesAin ShamsJAnaesthesiol73336 7108132 - 015828Sanj.etcNo ratings yet
- Anaesthesia For Major Abdominal SurgeryDocument1 pageAnaesthesia For Major Abdominal SurgerySanj.etcNo ratings yet
- IV Fluid ChartDocument2 pagesIV Fluid Charthady920No ratings yet
- Saline IV Fluid ComparisonDocument2 pagesSaline IV Fluid ComparisonSanj.etcNo ratings yet
- 01 15 DAS Algorithms Web PRINT20092015Document6 pages01 15 DAS Algorithms Web PRINT20092015Sanj.etcNo ratings yet
- SSCBundleCard PrintDocument2 pagesSSCBundleCard PrintSanj.etcNo ratings yet
- Emergency Laparotomy: Patient Information FactsheetDocument4 pagesEmergency Laparotomy: Patient Information FactsheetMuhammad RizqiNo ratings yet
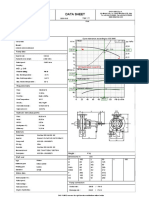
- Data Sheet: Item N°: Curve Tolerance According To ISO 9906Document3 pagesData Sheet: Item N°: Curve Tolerance According To ISO 9906Aan AndianaNo ratings yet
- Zilog Z80-SIO Technical Manual TextDocument58 pagesZilog Z80-SIO Technical Manual Textprada.rizzoplcNo ratings yet
- Dimmable Bulbs SamplesDocument11 pagesDimmable Bulbs SamplesBOSS BalaNo ratings yet
- Introduction To SCRDocument19 pagesIntroduction To SCRAlbin RobinNo ratings yet
- Phase DiagramDocument3 pagesPhase DiagramTing TCNo ratings yet
- Graduate Macro Theory II: The Real Business Cycle Model: Eric Sims University of Notre Dame Spring 2017Document25 pagesGraduate Macro Theory II: The Real Business Cycle Model: Eric Sims University of Notre Dame Spring 2017Joab Dan Valdivia CoriaNo ratings yet
- Gr. 10 Persuasive EssayDocument22 pagesGr. 10 Persuasive EssayZephania JandayanNo ratings yet
- Fcu Valve Honeywel PDFDocument6 pagesFcu Valve Honeywel PDFRyn YahuFNo ratings yet
- DLPFBSDocument1 pageDLPFBSEdnaMarquezMoralesNo ratings yet
- DICKSON KT800/802/803/804/856: Getting StartedDocument6 pagesDICKSON KT800/802/803/804/856: Getting StartedkmpoulosNo ratings yet
- Torrent - WSCC - Windows System Control Center 7.0.5.7 Commercial (x64 x86) - TeamOS - Team OS - Your Only Destination To Custom OS !!Document5 pagesTorrent - WSCC - Windows System Control Center 7.0.5.7 Commercial (x64 x86) - TeamOS - Team OS - Your Only Destination To Custom OS !!moustafaNo ratings yet
- ANSI AAMI ST63 2002 - Sterilization of Healthcare Products - Dry HeatDocument54 pagesANSI AAMI ST63 2002 - Sterilization of Healthcare Products - Dry HeatGraciane TagliettiNo ratings yet
- Activity 2Document5 pagesActivity 2DIOSAY, CHELZEYA A.No ratings yet
- Workplace Risk Assessment PDFDocument14 pagesWorkplace Risk Assessment PDFSyarul NizamzNo ratings yet
- Florida Motor Fuel Tax Relief Act of 2022Document9 pagesFlorida Motor Fuel Tax Relief Act of 2022ABC Action NewsNo ratings yet
- Company Profile PT. Geo Sriwijaya NusantaraDocument10 pagesCompany Profile PT. Geo Sriwijaya NusantaraHazred Umar FathanNo ratings yet
- Aquinas Five Ways To Prove That God Exists - The ArgumentsDocument2 pagesAquinas Five Ways To Prove That God Exists - The ArgumentsAbhinav AnandNo ratings yet
- EE 8602 - Protection and Switchgear Unit I - MCQ BankDocument11 pagesEE 8602 - Protection and Switchgear Unit I - MCQ Bankpoonam yadavNo ratings yet
- TOA Project Presentation (GROUP 5)Document22 pagesTOA Project Presentation (GROUP 5)Khadija ShahidNo ratings yet
- Jazz PrepaidDocument4 pagesJazz PrepaidHoney BunnyNo ratings yet
- Analysis of Green Entrepreneurship Practices in IndiaDocument5 pagesAnalysis of Green Entrepreneurship Practices in IndiaK SrivarunNo ratings yet
- Pre Intermediate Talking ShopDocument4 pagesPre Intermediate Talking ShopSindy LiNo ratings yet
- Pressure-Dependent Leak Detection Model and Its Application To A District Water SystemDocument13 pagesPressure-Dependent Leak Detection Model and Its Application To A District Water SystemManjul KothariNo ratings yet
- Lab Final SolutionDocument18 pagesLab Final SolutionZeeNo ratings yet
- Plane TrigonometryDocument545 pagesPlane Trigonometrygnavya680No ratings yet
- Watershed Conservation of Benguet VisDocument2 pagesWatershed Conservation of Benguet VisInnah Agito-RamosNo ratings yet
- VPZ M BrochureDocument2 pagesVPZ M BrochuresundyaNo ratings yet
- Technical Test 03Document13 pagesTechnical Test 03KartikNo ratings yet