You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- PSW Immunization MSDocument2 pagesPSW Immunization MSAngelica Mae FrialaNo ratings yet
- Dengue Pregnancy PDFDocument2 pagesDengue Pregnancy PDFSuhayatra PutraNo ratings yet
- Radioimmunoassay (RIA) Is An: in Vitro Antigens Hormone Blood BioassayDocument16 pagesRadioimmunoassay (RIA) Is An: in Vitro Antigens Hormone Blood BioassayDawlat SlamaNo ratings yet
- Guidelines For The Use of Fresh-Frozen Plasma, CryoprecipitateDocument18 pagesGuidelines For The Use of Fresh-Frozen Plasma, CryoprecipitatemelaniefarahdillaNo ratings yet
- AMENDMENT DIRECTIVE TO CONTROL COVID 19 PANDEMIC No 933 2022 EthiopiaDocument3 pagesAMENDMENT DIRECTIVE TO CONTROL COVID 19 PANDEMIC No 933 2022 EthiopiaAhmed AdemNo ratings yet
- Covid-19 Test Report PositiveDocument1 pageCovid-19 Test Report PositiveAbhinav PaikNo ratings yet
- Vaccination in PregnancyDocument7 pagesVaccination in PregnancyNoraNo ratings yet
- English Essay Topics on COVID-19 PandemicDocument4 pagesEnglish Essay Topics on COVID-19 Pandemicmaria evangelistaNo ratings yet
- Common Viral Exanthemas (Measles, Chickenpox & Rubella) : DR Sarika Gupta (MD, PHD), Assistant ProfessorDocument52 pagesCommon Viral Exanthemas (Measles, Chickenpox & Rubella) : DR Sarika Gupta (MD, PHD), Assistant ProfessorashighaNo ratings yet
- Discuss The Role of Immunology in SurgeryDocument16 pagesDiscuss The Role of Immunology in SurgeryrosybashNo ratings yet
- FILIRIASISDocument25 pagesFILIRIASISJoy Gao-ayNo ratings yet
- Swapan Kumar Nath Sanjay G Revankar Problem-Based PDFDocument1,163 pagesSwapan Kumar Nath Sanjay G Revankar Problem-Based PDFRestu100% (1)
- White Blood Cells: The Immune System's DefendersDocument1 pageWhite Blood Cells: The Immune System's DefendersSulochana ChanNo ratings yet
- Sample Tweets - ZikaDocument151 pagesSample Tweets - ZikaAlisonNo ratings yet
- Respiratory Tract InfectionsDocument17 pagesRespiratory Tract InfectionsPriya bhattiNo ratings yet
- Chicken Pox PresentationDocument14 pagesChicken Pox Presentationnur syafiqah kamaruzaman100% (3)
- Annotated BibliographyDocument7 pagesAnnotated Bibliographyapi-202202577No ratings yet
- Perbedaan Papila Dan Folikel Pada MataDocument2 pagesPerbedaan Papila Dan Folikel Pada MataMuhammad Agus Nashir100% (1)
- 2018-Pratiwi-J App Pharm SciDocument7 pages2018-Pratiwi-J App Pharm ScirizalNo ratings yet
- Techniques For Immune Function Analysis HandbookDocument248 pagesTechniques For Immune Function Analysis HandbookDante AvilésNo ratings yet
- 2018 - 07-TTI-Quarterly-Report-Form - 2nd QuarterDocument2 pages2018 - 07-TTI-Quarterly-Report-Form - 2nd QuarterRoy PasadillaNo ratings yet
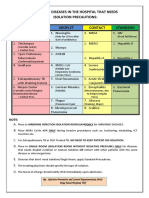
- Common Hospital Diseases Requiring Isolation PrecautionsDocument1 pageCommon Hospital Diseases Requiring Isolation Precautionsjerimiah_manzonNo ratings yet
- Barangay Monthly Inventory of Vaccinated PopulationDocument2 pagesBarangay Monthly Inventory of Vaccinated PopulationGenzo TaniaNo ratings yet
- 1) Bacterial Skin InfDocument32 pages1) Bacterial Skin InfsmrutuNo ratings yet
- University of Texas Medical School Book ListDocument6 pagesUniversity of Texas Medical School Book Listcamcas21No ratings yet
- Acinetobacter Ursingii Masquerading As Gram-Positive CocciDocument2 pagesAcinetobacter Ursingii Masquerading As Gram-Positive CocciMiguel CarlosNo ratings yet
- Collection, Handling and Labeling of Specimen ProtocolDocument2 pagesCollection, Handling and Labeling of Specimen ProtocolMEDLAB WOODLANDSNo ratings yet
- Antibody StructureDocument9 pagesAntibody StructureNikhil BijuNo ratings yet
- Molecular Virology, 2013 Edition (PDF) (DR - Carson) VRG PDFDocument1,013 pagesMolecular Virology, 2013 Edition (PDF) (DR - Carson) VRG PDFYuridia Rodríguez100% (3)
- Laboratory - Handbook - For - Clinicians Rearding HIV Testing SMS Medical College, JaipurDocument9 pagesLaboratory - Handbook - For - Clinicians Rearding HIV Testing SMS Medical College, Jaipurdileep2000No ratings yet