You might also like
- PPT Pe Baruuuu Yg Dibawa MajuuuDocument42 pagesPPT Pe Baruuuu Yg Dibawa MajuuuNaomiRimaClaudyaNo ratings yet
- Isrn Urology2012-707329 PDFDocument6 pagesIsrn Urology2012-707329 PDFNaomiRimaClaudyaNo ratings yet
- " Drop Foot": Arranged By: Nabiilah Aznesia NPM 71170891191Document12 pages" Drop Foot": Arranged By: Nabiilah Aznesia NPM 71170891191NaomiRimaClaudyaNo ratings yet
- Lien/Splen/Limpa: Oleh: Naomi R. Claudya Napitupulu 213210169 FK UMI 2013Document36 pagesLien/Splen/Limpa: Oleh: Naomi R. Claudya Napitupulu 213210169 FK UMI 2013NaomiRimaClaudyaNo ratings yet
- Entomologi RevisiDocument45 pagesEntomologi RevisiNaomiRimaClaudyaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- GenpathDocument8 pagesGenpathNatural Science BiologyNo ratings yet
- Major Depressive Disorder Symptoms and Prevalence For IB Abnormal PsychologyDocument13 pagesMajor Depressive Disorder Symptoms and Prevalence For IB Abnormal PsychologychrissybissyNo ratings yet
- Grand Case Presentation InformationDocument7 pagesGrand Case Presentation InformationCristina L. JaysonNo ratings yet
- LESSON 3: Exercise Variables and PrinciplesDocument31 pagesLESSON 3: Exercise Variables and PrinciplesCapulong Kimberly100% (1)
- Bioengineering Transla Med - 2022 - Chopade - Alzheimer S and Parkinson S Disease Therapies in The ClinicDocument23 pagesBioengineering Transla Med - 2022 - Chopade - Alzheimer S and Parkinson S Disease Therapies in The ClinicurosNo ratings yet
- Multiple Personality Disorder: Is It Fact or Fiction?: Deguzman 1Document10 pagesMultiple Personality Disorder: Is It Fact or Fiction?: Deguzman 1Eliza Philline De GuzmanNo ratings yet
- PhobiaDocument4 pagesPhobiaZeba QuadiriNo ratings yet
- Parasitology: - IntroductionDocument62 pagesParasitology: - IntroductionHana AliNo ratings yet
- Diabetic Nephropathy BaruDocument24 pagesDiabetic Nephropathy BaruRobiyanti Nur Chalifah HattaNo ratings yet
- Kleptomania Term PaperDocument6 pagesKleptomania Term Paperbctfnerif100% (1)
- SP42 Thoracentesis (Adult)Document7 pagesSP42 Thoracentesis (Adult)Adam HuzaibyNo ratings yet
- Evaluation of Bacterial Agents Isolated From Aspirate Cultures of Covid 19 General Intensivecare Patients Compared To Pre Pandemic ConditionsDocument8 pagesEvaluation of Bacterial Agents Isolated From Aspirate Cultures of Covid 19 General Intensivecare Patients Compared To Pre Pandemic ConditionsRicardo ZúñigaNo ratings yet
- Ultrasound Thesis TopicsDocument6 pagesUltrasound Thesis Topicsdw9x1bxb100% (2)
- Is Doa 10 Cup TestDocument1 pageIs Doa 10 Cup TestUqi.No ratings yet
- TramadolDocument2 pagesTramadolJordanne EtisNo ratings yet
- Newborn CareDocument19 pagesNewborn CareYa Mei LiNo ratings yet
- TicksDocument1 pageTicksTheChronicleHeraldNo ratings yet
- Skull Fracture Vs SuturesDocument6 pagesSkull Fracture Vs Suturesmohit372No ratings yet
- NCPDocument2 pagesNCPfierfizNo ratings yet
- ShockDocument53 pagesShockHassan Ahmed100% (3)
- An Approach To A Floppy InfantDocument33 pagesAn Approach To A Floppy InfantayunisallehNo ratings yet
- Endodontics Pain Control in Endodontics: Differential Diagnosis of Dental PainDocument4 pagesEndodontics Pain Control in Endodontics: Differential Diagnosis of Dental Painريام الموسويNo ratings yet
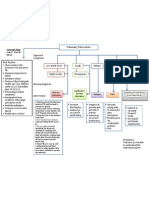
- Concept Map PTBDocument1 pageConcept Map PTBJoan Abardo100% (2)
- Bacteria Found in UrineDocument7 pagesBacteria Found in UrineAria DomingoNo ratings yet
- NephrologyDocument9 pagesNephrologyEliDavidNo ratings yet
- McWilliams Center For Counseling, Inc. Community Support Office - 438Document2 pagesMcWilliams Center For Counseling, Inc. Community Support Office - 438James BennettNo ratings yet
- Comparative Efficacy and Acceptability META-ANALYSIS 2015Document11 pagesComparative Efficacy and Acceptability META-ANALYSIS 2015Alexandra CastellanosNo ratings yet
- 103, Kanakia - B. Zillion Building, Lbs Marg, Kurla (W), Mumbai - 400 070Document10 pages103, Kanakia - B. Zillion Building, Lbs Marg, Kurla (W), Mumbai - 400 0708460074686No ratings yet
- APA Practice Guideline For The Treatment of Patients With Substance Use DisordersDocument276 pagesAPA Practice Guideline For The Treatment of Patients With Substance Use DisordersRaja Ahmad Rusdan MusyawirNo ratings yet
- Textbook of Gynaecological OncologyDocument58 pagesTextbook of Gynaecological OncologyMarco Vinicio Benavides Osorto100% (2)