You might also like
- Geriatrics Eval Management Tool For FrailtyDocument2 pagesGeriatrics Eval Management Tool For FrailtyDaulat JosuaNo ratings yet
- AdvairDocument1 pageAdvairE50% (2)
- Anemia Concept Mapping. Group 1Document82 pagesAnemia Concept Mapping. Group 1Giselle EstoquiaNo ratings yet
- Ati Med SurgDocument36 pagesAti Med SurgVanessaMUeller94% (17)
- Sign & Symptoms of Diseases: OM Nursing Academy Anil KantiwalDocument5 pagesSign & Symptoms of Diseases: OM Nursing Academy Anil KantiwalMudasir Ahmad BhatNo ratings yet
- Asthma ClassificationDocument1 pageAsthma ClassificationYak NafarNo ratings yet
- Pulm Audio Lecture Asthma Assessment SlidesDocument13 pagesPulm Audio Lecture Asthma Assessment SlidesSlyne CenarosaNo ratings yet
- Asthma Case StudyDocument39 pagesAsthma Case StudyDimitris TasiouNo ratings yet
- Asthma ZENDocument57 pagesAsthma ZENKonjit MitikuNo ratings yet
- Dr. Ediyono SP P Sub Dep Paru RSAL DR Ramelan: UHT September 2012Document50 pagesDr. Ediyono SP P Sub Dep Paru RSAL DR Ramelan: UHT September 2012gabyNo ratings yet
- Bronchial Asthma VERDEDocument83 pagesBronchial Asthma VERDEVanessa YunqueNo ratings yet
- Asthma by Ikmal WahabDocument19 pagesAsthma by Ikmal WahabIkmal WahabNo ratings yet
- ASTHMADocument41 pagesASTHMARobert L G MabongaNo ratings yet
- Ce Este Astmul?: Dr. Lavinia DavidescuDocument17 pagesCe Este Astmul?: Dr. Lavinia DavidescuStirNo ratings yet
- Pulmonary Disorders in PregnancyDocument49 pagesPulmonary Disorders in PregnancyMara Medina - BorleoNo ratings yet
- Asthma Diagnosis and Treatment GuidelineDocument20 pagesAsthma Diagnosis and Treatment GuidelineaanNo ratings yet
- Day 3Document5 pagesDay 3Royston NettoNo ratings yet
- Asthma: Kaps PrepDocument21 pagesAsthma: Kaps PrepImee TingzonNo ratings yet
- Asthma: Presentation By: Dr. Zunaira Nawaz Dr. Nida ShafiqueDocument47 pagesAsthma: Presentation By: Dr. Zunaira Nawaz Dr. Nida ShafiqueMohammad AliNo ratings yet
- WK6 Asthma Assignment Student VersionDocument8 pagesWK6 Asthma Assignment Student Versionnalit1985No ratings yet
- Paediatricshouseofficerguidehospitalkulim 151026150042 Lva1 App6891Document14 pagesPaediatricshouseofficerguidehospitalkulim 151026150042 Lva1 App6891Nadia SalwaniNo ratings yet
- Bronchial AsthmaDocument11 pagesBronchial AsthmaVishva Lalitbhai Hirpara100% (1)
- Pharmacotherapy of AsthmaDocument53 pagesPharmacotherapy of AsthmaStella Aprilia NurNo ratings yet
- PEF Variability Day S Highest PEF Lowest MeanDocument1 pagePEF Variability Day S Highest PEF Lowest MeanPhoebe SuboNo ratings yet
- Pharmacotherapy of Asthma: Asniar Pascayantri, S.Si., M.Si., AptDocument27 pagesPharmacotherapy of Asthma: Asniar Pascayantri, S.Si., M.Si., AptLeni Fitriani HamduNo ratings yet
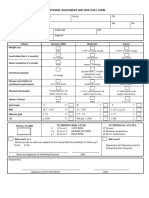
- 4 - Nutritional Assessment and Risk LevelDocument1 page4 - Nutritional Assessment and Risk LevelBok MatthewNo ratings yet
- Class 8 (09.08.2022)Document75 pagesClass 8 (09.08.2022)Ãqûã FîggâNo ratings yet
- Managing Asthma During Pregnancy and Lactation: Mary Mcmahon, RNC, MsDocument61 pagesManaging Asthma During Pregnancy and Lactation: Mary Mcmahon, RNC, MsIlya RosdianaNo ratings yet
- Stepwise Approach in Longterm Management of Asthma in ChildrenDocument41 pagesStepwise Approach in Longterm Management of Asthma in ChildrenAris BayuNo ratings yet
- REVISED-Med TaperingDocument3 pagesREVISED-Med TaperingDwi HerawatiNo ratings yet
- Difficult To Manage Asthma 2016Document69 pagesDifficult To Manage Asthma 2016muthia saniNo ratings yet
- Is Asthma Still A Risk Factor For General Anesthesia: Journal of AnesthesiologyDocument5 pagesIs Asthma Still A Risk Factor For General Anesthesia: Journal of AnesthesiologyRahadian MalikNo ratings yet
- Bronchiolitis PathwayDocument37 pagesBronchiolitis PathwayjerejerejereNo ratings yet
- Mild Moderate Severe Subset: Respiratory Arrest ImminentDocument7 pagesMild Moderate Severe Subset: Respiratory Arrest ImminentPia VSNo ratings yet
- As Ma 3Document27 pagesAs Ma 3chiajungNo ratings yet
- Asthma: A. DefinitionDocument6 pagesAsthma: A. DefinitionElvando SimatupangNo ratings yet
- If Yes To Any Question, Go To STEP 2: Table 2Document2 pagesIf Yes To Any Question, Go To STEP 2: Table 2Chelo Jan GeronimoNo ratings yet
- Suspected COVID-19 Cases Management in Triage HospitalsDocument6 pagesSuspected COVID-19 Cases Management in Triage HospitalsMuhamed RamadanNo ratings yet
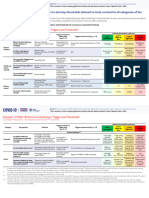
- Annex 1 - COVID 19 Alert Level System in Resource Constrained Settings - FINALDocument9 pagesAnnex 1 - COVID 19 Alert Level System in Resource Constrained Settings - FINALriclachicaNo ratings yet
- Glasgow Modified Alcohol Withdrawal ScaleDocument5 pagesGlasgow Modified Alcohol Withdrawal ScaleRichard SymondsNo ratings yet
- Medicine OSCE - Common Diseases Ver1Document4 pagesMedicine OSCE - Common Diseases Ver1TrisNo ratings yet
- NAEPP EPR-3 Classifi Cation of Asthma Severity & Control in Children 0-4 Years of AgeDocument1 pageNAEPP EPR-3 Classifi Cation of Asthma Severity & Control in Children 0-4 Years of AgeAdriel Chandra AngNo ratings yet
- G IN A: Lobal Itiative For SthmaDocument66 pagesG IN A: Lobal Itiative For SthmaNerissaArvianaShintaraNo ratings yet
- NCP Kasus 5Document9 pagesNCP Kasus 5Inne PratidinaNo ratings yet
- Epilepsy Education Prescribing Rubrics FINALDocument40 pagesEpilepsy Education Prescribing Rubrics FINALsamuelNo ratings yet
- Drug StudyDocument12 pagesDrug Studyjoaqiun100% (1)
- Aminoglycoside Guideline For Children-2Document7 pagesAminoglycoside Guideline For Children-2Alina CaraciobanuNo ratings yet
- NIH PocketGuideDocument16 pagesNIH PocketGuideOlga CîrsteaNo ratings yet
- ASTHMADocument36 pagesASTHMAKai Edmond MarvellaNo ratings yet
- Illness Trajectory in Palliative Care: SudirmanDocument62 pagesIllness Trajectory in Palliative Care: SudirmanMarlina SaputriNo ratings yet
- TreatmentProtocol 10-4-2021Document3 pagesTreatmentProtocol 10-4-2021Anishk SinghNo ratings yet
- Asma Current Family MedicineDocument7 pagesAsma Current Family MedicineRay Erick RamosNo ratings yet
- Clinical Global Impressions (Cgi)Document2 pagesClinical Global Impressions (Cgi)Ejournal100% (1)
- DexamethasoneDocument1 pageDexamethasoneACOB, Jamil C.No ratings yet
- Asma Bronkiale: Muhsin Ppds Ilmu Penyakit Dalam FK Unsyiah Pembimbing: Dr. T. Mamfaluti, M.Kes, SP - PD, FinasimDocument33 pagesAsma Bronkiale: Muhsin Ppds Ilmu Penyakit Dalam FK Unsyiah Pembimbing: Dr. T. Mamfaluti, M.Kes, SP - PD, FinasimEvy LiesniawatiNo ratings yet
- Overview of Asthma Management: Zeshan Haider Kazmi M.Phil (Pharmacology)Document49 pagesOverview of Asthma Management: Zeshan Haider Kazmi M.Phil (Pharmacology)chiajungNo ratings yet
- Bronchial Asthma: Mariam Lwasa Naluwugge Afrah 215-083011-07387Document25 pagesBronchial Asthma: Mariam Lwasa Naluwugge Afrah 215-083011-07387NinaNo ratings yet
- Obstructive Pulmonary DiseasesDocument50 pagesObstructive Pulmonary DiseasesGopala HariNo ratings yet
- Asthma: Chronic Inflammatory Airway DiseaseDocument14 pagesAsthma: Chronic Inflammatory Airway DiseaseyyNo ratings yet
- Supplementary Material 1a Acute AsthmaDocument3 pagesSupplementary Material 1a Acute AsthmaANGELIE CRISTINE POMADONo ratings yet
- Sign and SymptomsDocument5 pagesSign and Symptomsmadras meditationNo ratings yet
- Chemotherapy Side Effects WorksheetDocument6 pagesChemotherapy Side Effects Worksheetreny hartikasariNo ratings yet
- Overcoming Depression The Quick Guide to Leaving Depression to Cheerfulness in 2 HoursFrom EverandOvercoming Depression The Quick Guide to Leaving Depression to Cheerfulness in 2 HoursNo ratings yet
- Able of Ontents: EdiatricsDocument4 pagesAble of Ontents: EdiatricsDrx ahmed MaherNo ratings yet
- 2-6 Book-2Document400 pages2-6 Book-2Drx ahmed MaherNo ratings yet
- Presentation TipsDocument4 pagesPresentation TipsDrx ahmed MaherNo ratings yet
- Types of Economic and Humanistic Outcomes Assessments: Kathleen M. Bungay, Pharm.D. and Lisa A. Sanchez, Pharm.DDocument48 pagesTypes of Economic and Humanistic Outcomes Assessments: Kathleen M. Bungay, Pharm.D. and Lisa A. Sanchez, Pharm.DDrx ahmed MaherNo ratings yet
- Types of Economic and Humanistic Outcomes Assessments: Kathleen M. Bungay, Pharm.D. and Lisa A. Sanchez, Pharm.DDocument48 pagesTypes of Economic and Humanistic Outcomes Assessments: Kathleen M. Bungay, Pharm.D. and Lisa A. Sanchez, Pharm.DDrx ahmed MaherNo ratings yet
- RecertificationDocument10 pagesRecertificationDrx ahmed MaherNo ratings yet
- Candidates GuideDocument17 pagesCandidates GuideDrx ahmed MaherNo ratings yet
- 060 2Document31 pages060 2Drx ahmed MaherNo ratings yet
- 040 1Document44 pages040 1Drx ahmed MaherNo ratings yet
- 080 3Document44 pages080 3Drx ahmed MaherNo ratings yet
- 070 2Document31 pages070 2Drx ahmed MaherNo ratings yet
- 070 1Document24 pages070 1Drx ahmed MaherNo ratings yet
- Conflict of Interest Disclosures: 2011 Updates in TherapeuticsDocument21 pagesConflict of Interest Disclosures: 2011 Updates in TherapeuticsDrx ahmed MaherNo ratings yet
- 080 2Document28 pages080 2Drx ahmed MaherNo ratings yet
- 060 3Document35 pages060 3Drx ahmed MaherNo ratings yet
- 050 3Document22 pages050 3Drx ahmed MaherNo ratings yet
- 2011 Updates in Therapeutics:: Conflict of Interest DisclosuresDocument14 pages2011 Updates in Therapeutics:: Conflict of Interest DisclosuresDrx ahmed MaherNo ratings yet
- 050 1Document38 pages050 1Drx ahmed MaherNo ratings yet
- Conflict of Interest Disclosures: 2011 Updates in TherapeuticsDocument34 pagesConflict of Interest Disclosures: 2011 Updates in TherapeuticsDrx ahmed MaherNo ratings yet
- Conflict of Interest Disclosures: 2011 Updates in TherapeuticsDocument39 pagesConflict of Interest Disclosures: 2011 Updates in TherapeuticsDrx ahmed MaherNo ratings yet
- 040 2Document26 pages040 2Drx ahmed MaherNo ratings yet
- Conflict of Interest Disclosures: 2011 Updates in TherapeuticsDocument34 pagesConflict of Interest Disclosures: 2011 Updates in TherapeuticsDrx ahmed MaherNo ratings yet
- Conflict of Interest Disclosures: Endocrine and Metabolic DisordersDocument32 pagesConflict of Interest Disclosures: Endocrine and Metabolic DisordersDrx ahmed MaherNo ratings yet
- Conflict of Interest Disclosures: 2011 Updates in TherapeuticsDocument24 pagesConflict of Interest Disclosures: 2011 Updates in TherapeuticsDrx ahmed MaherNo ratings yet
- Conflict of Interest Disclosure: 2011 Updates in TherapeuticsDocument19 pagesConflict of Interest Disclosure: 2011 Updates in TherapeuticsDrx ahmed MaherNo ratings yet
- OutlineDocument20 pagesOutlineDrx ahmed MaherNo ratings yet
- OutlineDocument20 pagesOutlineDrx ahmed MaherNo ratings yet
- Conflict of Interest DisclosuresDocument24 pagesConflict of Interest DisclosuresDrx ahmed MaherNo ratings yet
- 2011 Updates in Therapeutics: P P: The Pharmacotherapy Preparatory Review and Recertification CourseDocument11 pages2011 Updates in Therapeutics: P P: The Pharmacotherapy Preparatory Review and Recertification CourseDrx ahmed MaherNo ratings yet
- MGI - Prioritizing Health - Executive Summary - July 2020Document32 pagesMGI - Prioritizing Health - Executive Summary - July 2020Iful ScienceboyNo ratings yet
- NCK Examination Past Pps1,2,3,4-1Document59 pagesNCK Examination Past Pps1,2,3,4-1jimwao100% (1)
- COPD Physio-Pedia PDFDocument17 pagesCOPD Physio-Pedia PDFsazi01No ratings yet
- Respiratory Drugs XL Chart 3Document2 pagesRespiratory Drugs XL Chart 3cdp1587100% (1)
- Tamilnadu Board Class 11 Zoology Chapter 6Document22 pagesTamilnadu Board Class 11 Zoology Chapter 6Varshini PeraNo ratings yet
- Questions On Smoking Tobacco Use and HealthDocument4 pagesQuestions On Smoking Tobacco Use and HealthJay marie enriquezNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument8 pagesChronic Obstructive Pulmonary DiseaseYessamin Paith RoderosNo ratings yet
- Activity-11-Respiratory-System - PERALTADocument3 pagesActivity-11-Respiratory-System - PERALTACogie PeraltaNo ratings yet
- Mechanical Ventilation of Adults in The Emergency Department - UpToDateDocument28 pagesMechanical Ventilation of Adults in The Emergency Department - UpToDateCarlos E. Morales AyoraNo ratings yet
- Module 3 21BE45 Biology For Engineers 28 PagesDocument33 pagesModule 3 21BE45 Biology For Engineers 28 PagesManasa ManasaNo ratings yet
- Continuous Positive Airway Pressure (CPAP)Document9 pagesContinuous Positive Airway Pressure (CPAP)yassen hassanNo ratings yet
- Anatomy and Physiology by Dennis Munoz2Document1,273 pagesAnatomy and Physiology by Dennis Munoz2Dennis Nabor Muñoz, RN,RMNo ratings yet
- Serrato Joshua Stephen D Health g10 q2 w8 LasDocument5 pagesSerrato Joshua Stephen D Health g10 q2 w8 Lasjoshua tejadaNo ratings yet
- 1.chronic Illness Overview and COPDDocument12 pages1.chronic Illness Overview and COPDOmar IzzoNo ratings yet
- A Nurse Is Preparing To Obtain A Sputum Specimen From A Male ClientDocument32 pagesA Nurse Is Preparing To Obtain A Sputum Specimen From A Male ClientSophia Veron50% (2)
- p173 PDFDocument8 pagesp173 PDFKarinaWijayantiNo ratings yet
- Sample Review Questions in Medical and Surgical Nursing and Sample Board Exam QuestionsDocument22 pagesSample Review Questions in Medical and Surgical Nursing and Sample Board Exam Questionstinea nigraNo ratings yet
- PhysioEx9,1: Exercise 7 Activity 2: PEX-07-02Document8 pagesPhysioEx9,1: Exercise 7 Activity 2: PEX-07-02mishael_baig100% (11)
- Brochure PDFDocument16 pagesBrochure PDFFebinNo ratings yet
- Environmental Pollution FinalDocument45 pagesEnvironmental Pollution FinalReganNo ratings yet
- Juliana Tambellini: University of PittsburghDocument19 pagesJuliana Tambellini: University of PittsburghzackNo ratings yet
- PATIENT 1 Nursing Assessment FormDocument5 pagesPATIENT 1 Nursing Assessment FormndemboloveNo ratings yet
- Stability Indicating RP-HPLC Method For The Determination of Terbutaline Sulphate, Guaifenesin, Ambroxol Hydrochloride and Preservatives Content in Liquid FormulationsDocument6 pagesStability Indicating RP-HPLC Method For The Determination of Terbutaline Sulphate, Guaifenesin, Ambroxol Hydrochloride and Preservatives Content in Liquid FormulationsHanimi ReddyNo ratings yet
- Gold 2019Document43 pagesGold 2019Hayatillah Natasya100% (1)
- Aacvpr GuidelinesDocument36 pagesAacvpr GuidelinesChitrang AmonkarNo ratings yet
- Lungs - Facts, Function and Diseases - Live ScienceDocument12 pagesLungs - Facts, Function and Diseases - Live ScienceImtiax LaghariNo ratings yet