You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- 4 5969910185303475765 PDFDocument116 pages4 5969910185303475765 PDFEdy Tahir MattoreangNo ratings yet
- Gambaran CT SCAN: (Kasus: Edh, SDH, Ich, Sah, Infark Cerebri, IvhDocument44 pagesGambaran CT SCAN: (Kasus: Edh, SDH, Ich, Sah, Infark Cerebri, Ivhfahmi rosyadiNo ratings yet
- Empirical First Line AntibioticsDocument1 pageEmpirical First Line Antibioticsdiati zahrainiNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Sexually Transmitted InfectionsDocument110 pagesSexually Transmitted Infectionstummalapalli venkateswara raoNo ratings yet
- Obesity Exercise PrescriptionDocument34 pagesObesity Exercise Prescriptionkhushbu88% (8)
- A Mental Healthcare Model For Mass Trauma Survivors - M. Basoglu, Et. Al., (Cambridge, 2011) WW PDFDocument296 pagesA Mental Healthcare Model For Mass Trauma Survivors - M. Basoglu, Et. Al., (Cambridge, 2011) WW PDFraulNo ratings yet
- Monoclonal Antibodies and Engineered AntibodiesDocument24 pagesMonoclonal Antibodies and Engineered AntibodiesMunawar AliNo ratings yet
- Analytical Method Validation of Clopidogrel Tablets BR HPLCDocument48 pagesAnalytical Method Validation of Clopidogrel Tablets BR HPLCAman ThakurNo ratings yet
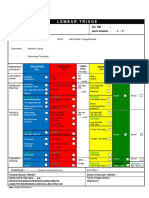
- Lembar Triage: Nama Pasien: Tanggal Lahir: No. RM: Jenis Kelamin: L / PDocument1 pageLembar Triage: Nama Pasien: Tanggal Lahir: No. RM: Jenis Kelamin: L / PEdy Tahir MattoreangNo ratings yet
- RagozineDocument28 pagesRagozineMoisés MedinaNo ratings yet
- Bergs2015 PDFDocument12 pagesBergs2015 PDFEdy Tahir MattoreangNo ratings yet
- Applied Ergonomics: Rebecca J. Mitchell, Ann Williamson, Brett MolesworthDocument11 pagesApplied Ergonomics: Rebecca J. Mitchell, Ann Williamson, Brett MolesworthEdy Tahir MattoreangNo ratings yet
- The SSI BundleDocument15 pagesThe SSI BundleEdy Tahir MattoreangNo ratings yet
- Pone 0101915Document9 pagesPone 0101915Edy Tahir MattoreangNo ratings yet
- Corp Aorn Flyer Pdf2Document1 pageCorp Aorn Flyer Pdf2Edy Tahir MattoreangNo ratings yet
- Sacks Et Al. - 2015 - Teamwork, Communication and Safety Climate A Systematic Review of Interventions To Improve Surgical CultureDocument11 pagesSacks Et Al. - 2015 - Teamwork, Communication and Safety Climate A Systematic Review of Interventions To Improve Surgical CultureEdy Tahir MattoreangNo ratings yet
- Aorn 2016 - Wound Prevalence Study - 161092 Corp Aorn Poster Pdf3Document1 pageAorn 2016 - Wound Prevalence Study - 161092 Corp Aorn Poster Pdf3Edy Tahir MattoreangNo ratings yet
- The SSI BundleDocument15 pagesThe SSI BundleEdy Tahir MattoreangNo ratings yet
- Sacks Et Al. - 2015 - Teamwork, Communication and Safety Climate A Systematic Review of Interventions To Improve Surgical CultureDocument11 pagesSacks Et Al. - 2015 - Teamwork, Communication and Safety Climate A Systematic Review of Interventions To Improve Surgical CultureEdy Tahir MattoreangNo ratings yet
- Early Warning SystemDocument5 pagesEarly Warning SystemEdy Tahir MattoreangNo ratings yet
- WHO Dengue Guidelines 2013Document160 pagesWHO Dengue Guidelines 2013Jason MirasolNo ratings yet
- Handbook: For Clinical Management of DengueDocument124 pagesHandbook: For Clinical Management of DengueraattaiNo ratings yet
- HeyDocument1 pageHeyEdy Tahir MattoreangNo ratings yet
- Tugas Perilaku OrganisasiDocument20 pagesTugas Perilaku OrganisasiEdy Tahir MattoreangNo ratings yet
- Evaluation of scales in immune-mediated polyneuropathiesDocument222 pagesEvaluation of scales in immune-mediated polyneuropathiesAngelo MalerbaNo ratings yet
- Fycompa Efficacy Adjunctive Partial SeizuresDocument20 pagesFycompa Efficacy Adjunctive Partial SeizuresoneniravNo ratings yet
- The LungsDocument6 pagesThe LungsnandaNo ratings yet
- Unit 2Document4 pagesUnit 2api-296199660No ratings yet
- Anvisa National Health Surveillance AgencyDocument52 pagesAnvisa National Health Surveillance AgencyVimarsha HSNo ratings yet
- Excerpt: "Unaccountable: What Hospitals Won't Tell You and How Transparency Can Revolutionize Health Care" by Marty MakaryDocument4 pagesExcerpt: "Unaccountable: What Hospitals Won't Tell You and How Transparency Can Revolutionize Health Care" by Marty Makarywamu885No ratings yet
- Elgabri v. Lekas, M.D., 1st Cir. (1992)Document21 pagesElgabri v. Lekas, M.D., 1st Cir. (1992)Scribd Government DocsNo ratings yet
- Ayushman Bharat - KailashDocument11 pagesAyushman Bharat - KailashKailash NagarNo ratings yet
- ReviewerDocument20 pagesReviewerYang MolosNo ratings yet
- Elphos Erald: Second Shot: Hillary Clinton Running Again For PresidentDocument10 pagesElphos Erald: Second Shot: Hillary Clinton Running Again For PresidentThe Delphos HeraldNo ratings yet
- Hyperthermia and Risk For AspirationDocument3 pagesHyperthermia and Risk For AspirationAlmyr RimandoNo ratings yet
- 64 Vital Nerve CentresDocument29 pages64 Vital Nerve CentresadinaNo ratings yet
- IRB Definitions (Is It Research? and Definitions of Exempt, Expedited and Full)Document4 pagesIRB Definitions (Is It Research? and Definitions of Exempt, Expedited and Full)analyn123No ratings yet
- CCMP 2020 Batch Cardiovascular MCQsDocument2 pagesCCMP 2020 Batch Cardiovascular MCQsharshad patelNo ratings yet
- Expansion Screw Activation Guidelines PDFDocument1 pageExpansion Screw Activation Guidelines PDFOsama SayedahmedNo ratings yet
- Zocor (Simvastatin)Document3 pagesZocor (Simvastatin)E100% (1)
- Sound Transduction EarDocument7 pagesSound Transduction Earhsc5013100% (1)
- Resume Jurnal-Dessy Dwi H 201720401011160Document3 pagesResume Jurnal-Dessy Dwi H 201720401011160Pratiwi UmbohNo ratings yet
- ق 4Document36 pagesق 4Zainab HasanNo ratings yet
- Makalah Bahasa InggrisDocument2 pagesMakalah Bahasa InggrisOlga RevalinaNo ratings yet
- Medical Surgical Treatments For EDDocument31 pagesMedical Surgical Treatments For EDskumar_p7No ratings yet
- AcidifiersDocument17 pagesAcidifiersKarim Khalil100% (3)
- Large Volume Parenterals: Guidelines and Quality Control TestsDocument36 pagesLarge Volume Parenterals: Guidelines and Quality Control TestsRákêsh MãttàNo ratings yet