You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Paul Marik Vitamin C CHESTDocument10 pagesPaul Marik Vitamin C CHESTIrwan YongnardiNo ratings yet
- The McKenzie MethodDocument72 pagesThe McKenzie MethodDr-Gehad Samy Halwagy100% (3)
- Princess Arianne Macaranas Seven Hello Rache PracticeDocument2 pagesPrincess Arianne Macaranas Seven Hello Rache PracticeDianne MacaranasNo ratings yet
- Enteral Parenteral NutritionDocument80 pagesEnteral Parenteral NutritionJehangir AllamNo ratings yet
- Physiotherapy Treatment ScarsDocument3 pagesPhysiotherapy Treatment ScarsYuyun Aryuni MusrifNo ratings yet
- Case Study of Ruptured Appendicitis With Localize Peritonitis (Final)Document76 pagesCase Study of Ruptured Appendicitis With Localize Peritonitis (Final)DRJC82% (22)
- Aromatherapy, Massage PDFDocument233 pagesAromatherapy, Massage PDFGyarmati LászlóNo ratings yet
- What Cause of AsthmaDocument6 pagesWhat Cause of AsthmaLion KingNo ratings yet
- New PRC Form MidwiferyDocument4 pagesNew PRC Form MidwiferyJrr Estabaya Irang96% (27)
- Im Residency FlowchartDocument1 pageIm Residency FlowchartF Badruzzama BegumNo ratings yet
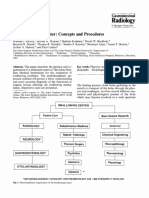
- 4.3 Swallowing - Center - Concepts - and - ProceduresDocument7 pages4.3 Swallowing - Center - Concepts - and - Proceduresluribe662No ratings yet
- 6-19 PRC v. de Guzman, G.R. No. 144681, June 21, 2004Document17 pages6-19 PRC v. de Guzman, G.R. No. 144681, June 21, 2004Reginald Dwight FloridoNo ratings yet
- Hepatosplenomegaly: - Question: - AnswerDocument7 pagesHepatosplenomegaly: - Question: - AnswerSyximsh FPNo ratings yet
- ACOG The RH Factor How It Can Affect Your Pregnancy PDFDocument3 pagesACOG The RH Factor How It Can Affect Your Pregnancy PDFdoc moNo ratings yet
- Resume-Parimala DeepthiDocument2 pagesResume-Parimala DeepthideeptiNo ratings yet
- Medical Specialty Recruitment Applicant Handbook 2021 v1.1Document50 pagesMedical Specialty Recruitment Applicant Handbook 2021 v1.1SamNo ratings yet
- Mri Referral Package For Axxess Imaging April 2020Document4 pagesMri Referral Package For Axxess Imaging April 2020JovanyGrezNo ratings yet
- Anaesthetic Case StudyDocument11 pagesAnaesthetic Case StudysomyntNo ratings yet
- Antimony Gluconate-1Document13 pagesAntimony Gluconate-1humag143100% (3)
- ChinaDocument57 pagesChinaAsaf NaeemNo ratings yet
- 1 Laporan Pengeluaran Obat Dan Alkes Depyan 28 SEPTEMBER 2019Document18 pages1 Laporan Pengeluaran Obat Dan Alkes Depyan 28 SEPTEMBER 2019Indah SetyowatiNo ratings yet
- RS PaperDocument12 pagesRS PaperGRAZ SHIEL HARINo ratings yet
- Final NPRD, 2021Document28 pagesFinal NPRD, 2021Maruthi RoshanNo ratings yet
- Mood Disorder OverviewDocument2 pagesMood Disorder OverviewAtoho SemaNo ratings yet
- Sacrifice 2Document8 pagesSacrifice 2Mainan AjalahNo ratings yet
- University of The Philippines Manila College of MedicineDocument3 pagesUniversity of The Philippines Manila College of MedicineDhian MorishitaNo ratings yet
- Scientific Research About Sea Moss PDFDocument2 pagesScientific Research About Sea Moss PDFHerbNo ratings yet
- Classroom Set-Up Food Vaccine FrequencyDocument5 pagesClassroom Set-Up Food Vaccine FrequencyLuke Edward PanganibanNo ratings yet
- Paracetamol Drug StudyDocument1 pageParacetamol Drug Studyrain peregrinoNo ratings yet
- Shingles RecombinantDocument2 pagesShingles Recombinantn99aliNo ratings yet